Abstract
This study reports a case of a 24-year-old female patient who presented with
recurrent palpitations over two months, accompanied by significantly reduced left
ventricular systolic function (LVEF of 22%) and pleural and peritoneal effusions.
An electrophysiological examination confirmed a diagnosis of tachycardia-induced
cardiomyopathy due to ventricular tachycardia originating from the left posterior
fascicle. She received a successful radiofrequency catheter ablation. One week later
the LVEF of this patient improved to 48%.
Keywords
INTRODUCTION
Left posterior fascicular ventricular tachycardia (LPFVT) is the most common form of idiopathic ventricular tachycardia and is characterized by a right bundle branch block (RBBB) pattern with left-axis deviation [1,2]. It predominantly affects young patients and is typically not associated with underlying structural heart disease. LPFVT generally responds well to calcium channel blockers, such as verapamil. Although the prognosis of LPFVT is usually favorable, recurrent episodes may result in tachycardia-induced cardiomyopathy, leading to progressive cardiac dysfunction. This case report presents the clinical diagnosis and management of a young female patient who developed arrhythmia-induced cardiomyopathy secondary to LPFVT, aiming to elucidate the diagnostic approach, therapeutic strategies, and prognosis of this disease.
CASE REPORT
Basic Patient Information
A 24-year-old female patient experienced recurrent episodes of palpitations over the past two months, accompanied by decreased exercise tolerance. Two days before admission, she developed more frequent palpitations. An electrocardiogram (ECG) revealed ventricular tachycardia (a ventricular rate of 157 beats per minute), and computed tomography (CT) demonstrated multiple and peritoneal effusions. Three months earlier, she had undergone tooth extraction complicated by a localized inflammatory response, for which she received a short course of oral cephalosporin antibiotics, with no other history of drug exposure. There was no family history of hereditary diseases. Aside from palpitations, she exhibited no additional clinical manifestations, such as syncope (Figure 1).
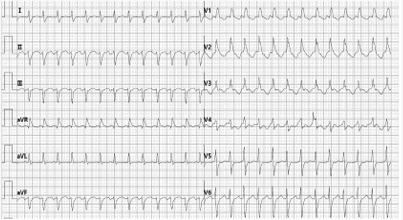
Figure 1: Electrocardiogram during an episode of ventricular tachycardia
Admission examination
The patient underwent comprehensive laboratory testing and imaging evaluations. Electrocardiography revealed ventricular tachycardia (VT) with QT intervalprolongation. Transthoracic echocardiography (TTE) revealed a left ventricular ejection fraction (LVEF) of 22%, left ventricular wall motion abnormalities, and impaired systolic function (left ventricular end-systolic diameter, LVESD=43 mm; left ventricular end-diastolic diameter, LVEDD=53 mm) without evidence of valvular or structural abnormalities. Holter monitoring identified recurrent episodes of nonsustained ventricular tachycardia and T-wave abnormalities with QT interval prolongation. Cardiac magnetic resonance imaging revealed no specific abnormalities, and no evidence of structural heart disease was observed. Serum high-sensitivity cardiac troponin T (hs-cTnT) was elevated (24.3 pg/ mL), and N-terminal pro-B-type natriuretic peptide (NT proBNP) was markedly increased (9418 pg/mL). The Ddimer level was 8.62 mg/L, with alanine aminotransferase (ALT) at 153 U/L and aspartate aminotransferase (AST) at 102 U/L. Other laboratory evaluations, including renal function, electrolyte panels, thyroid function tests, and coronary and pulmonary artery computed tomography (CTA), were unremarkable, excluding structural and metabolic etiologies (Figure 2).
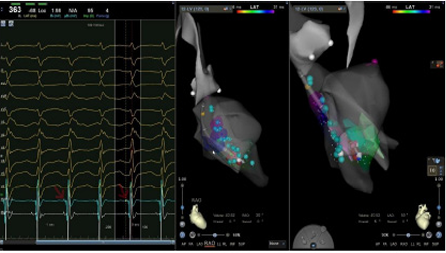
Figure 2: Target diagram (the premature P2 potential is at the arrow)
TREATMENT
After admission, the patient’s electrocardiogram demonstrated ventricular tachycardia, although hemodynamic stability was maintained. Intravenous verapamil was administered, the sinus rhythm was successfully restored, and anti-heart failure therapy was initiated. Within 24 hours, the patient experienced a recurrence of ventricular tachycardia, which was associated with hemodynamic instability. Synchronized direct current cardioversion (150 J) successfully restored sinus rhythm. On the second day of hospitalization, the patient again developed ventricular tachycardia. Synchronized cardioversion was attempted but failed to terminate the arrhythmia, and ventricular tachycardia persisted. Given the recurrent episodes and persistent cardiac dysfunction, an electrophysiological study (EPS) and radiofrequency catheter ablation (RFCA) were pursued (Figure3).
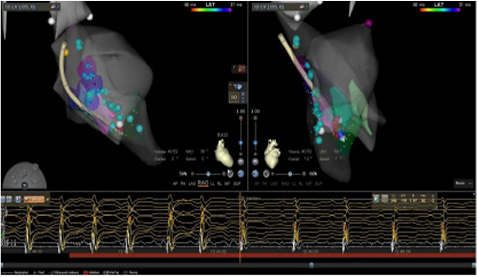
Figure 3: Ventricular Tachycardia disappeared after ablation procedure
With the guidance of intracardiac echocardiography (ICE), a three-dimensional anatomical model of the left ventricle was constructed. Subsequently, electroanatomical mapping of the His bundle, left posterior fascicle, and left anterior fascicle were performed using the CARTO3 system combined with a DecaNav decapolar high-density mapping catheter. Bipolar voltage mapping revealed an overall left ventricular voltage range of 0.36–1.98 mV without evidence of dense scarring. Programmed ventricular stimulation reproducibly induced wide QRS tachycardia with a typical RBBB morphology and left superior axis deviation, which was consistent with clinical tachycardia. Activation mapping revealed the earliest P2 potential at the mid-to-lower interventricular septum, corresponding to the distal portion of the left posterior fascicle. Based on these findings, an irrigated contact force-sensing catheter (SmartTouch-SF) was positioned slightly toward the basal side of the earliest P2 region. Radiofrequency energy (40 W, 27℃) was applied, resulting in the termination of tachycardia within 1 second of the initial ablation. After an additional 360 seconds of consolidation ablation, repeated programmed stimulation after intravenous bolus of isoprenaline (0.2%) failed to induce further ventricular tachycardia. A 30-minute observation period with repeated stimulation confirmed the success of the ablation (Figure 4).
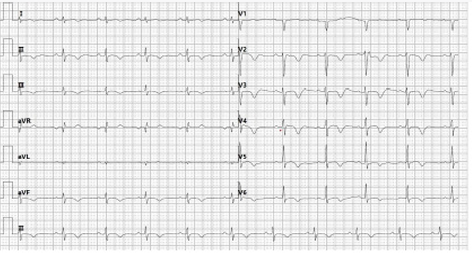
Figure 4: Electrocardiogram shows sinus rhythm after radiofrequency ablation
The first day after the RFCA, electrocardiography demonstrated sinus rhythm. One week later, transthoracic echocardiography revealed an LVEF of 48%, with notable recovery of left ventricular systolic function (LVESD was reduced to 35 mm; LVEDD was reduced to 48 mm). Follow-up chest computed tomography indicated resolution of the plural and peritoneal effusions. The NT-proBNP level decreased from 9418 pg/mL at admission to 606 pg/mL. The patient was discharged with all anti-heart failure medications and is currently under follow-up.
DISCUSSION
LPFVT is a form of idiopathic ventricular tachycardia that is typically driven by a reentrant circuit. The antegrade limb consists of slowly conducting, verapamil-sensitive fibers, whereas the retrograde limb involves conduction through the left posterior fascicle. The anatomical substrate underlying LPFVT has long been a subject of investigation. In a study involving 26 patients with LPFVT, all had false tendons (FTs) within the left ventricle, suggesting that FTs may serve as an electroanatomical substrate for LPFVT [3]. However, the pre cise mechanisms by which FTs facilitate ventricular tachy cardia remain incompletely understood. Some investigators propose that Purkinje fibers embedded within FTs form part of the reentrant circuit by providing a conduit for electrical conduction [4]. In contrast, others suggest that mechanical stretch and tension exerted by FTs at their attachment sites and adjacent Purkinje networks may trigger localized slow conduction or discrete reentry [3].
LPFVT is generally considered a benign condition. However, recurrent episodes of ventricular tachycardia can result in tachycardia-induced cardiomyopathy. In this case, the patient experienced recurrent palpitations, which were likely associated with prolonged episodes of ventricular tachycardia. Owing to the patient’s young age and relatively good tolerance, hospitalization was delayed until the development of more severe myocardial dysfunction accompanied by pleural and peritoneal effusions. Clinically, the presentation resembled dilated cardiomyopathy, with markedly impaired left ventricular function. During hospitalization, intravenous verapamil successfully restored sinus rhythm, confirming the sensitivity of LPFVT to verapamil. During EPS, ventricular S1S1 stimulation subsequently induced an entrainment phenomenon, further supporting a reentrant mechanism. Electroanatomical mapping localized the earliest activation site near the left posterior fascicle, and targeted radiofrequency ablation at this site successfully eliminated tachycardia. One week post ablation, the cardiac structural and functional abnormalities were reversed, and the plural and peritoneal effusions were completely resolved. The rapid recovery of cardiac function argues against a diagnosis of primary dilated cardiomyopathy. Based on the clinical course, laboratory findings, and electrophysiological findings, a final diagnosis of tachycardia-induced cardiomyopathy secondary to ventricular tachycardia originating from the left posterior fascicle was established.
Various forms of tachyarrhythmia can induce tachycardia-induced cardiomyopathy (TIC), and previous case reports have documented different types of arrhythmias leading to its development [5,6]. VT markedly increases myocardial oxygen consumption by maintaining a persistently high ventricular rate while concomitantly shortening diastole, thereby reducing coronary perfusion time and precipitating myocardial ischemia and disturbances in energy metabolism [7]. Chronic energy depletion and oxidative stress trigger cardiomyocyte apoptosis and necrosis, activate inflammatory pathways, stimulate fibroblast proliferation and extracellular matrix remodeling, and ultimately lead to ventricular dilatation and impaired systolic function [8]. Studies have shown that, in patients with TIC, the reduction in LVEF is positively correlated with both the duration and frequency of ventricular tachycardia [9]. Moreover, Ulus et al. delineated three sequential stages in the evolution of tachycardia-induced cardiomyopathy. During the initial compensatory phase, which lasts approximately one week, left ventricular pump performance remains preserved; however, the sympathetic–neurohormonal axis is activated, and early alterations in the extracellular matrix emerge. In the second phase, cellular remodeling and contractile dysfunction arise, leading to progressive left ventricular systolic impairment and dilation, accompanied by sustained upregulation of the renin‒angiotensin system. In the final heart failure phase, severe left ventricular pump failure and pronounced dilation occur, with marked neuroendocrine overactivation that culminates in systemic hemodynamic compromise and both pulmonary and systemic congestion [10]. Although elevated B-type natriuretic peptide (BNP) concentrations represent a compensatory response, persistently high BNP levels indicate increased wall stress and are closely associated with an adverse prognosis [11]. Studies also suggest that sustained ventricular tachycardia can cause diffuse left ventricular dilatation and heightened wall stress. In contrast, reverse remodeling may occur within 3–6 months after tachycardia is eliminated by cardioversion or catheter ablation [9].
The primary goals of TIC management are to restore sinus rhythm whenever possible, control the ventricular rate, alleviate heart failure symptoms, reverse cardiac remodeling, and prevent recurrence. Catheter-based radiofrequency ablation is the most effective treatment for ventricular tachycardia-related cardiomyopathy [12]. Previous case reports indicate that persistent ventricular tachycardia precipitates maladaptive myocardial remodeling and sympathetic neural remodeling [13]. The RFCA for tachycardia-induced cardiomyopathy has been shown to reverse both sympathetic remodeling and structural alterations of the myocardium [14]. Notably, the success of ablation depends not only on precise electrophysiological localization but also on comprehensive analysis of overall electrophysiological activity. Recent studies have suggested that the left posterior fascicle may not always represent the critical origin of LPFVT [15]. In some cases, it may merely serve as a “bystander.” Therefore, during ablation, attention must extend beyond the left posterior fascicle to encompass the entire Purkinje network to eliminate the pathological circuit completely. Typically, ablation targeting the Purkinje (P) potential achieves a high success rate with a low recurrence rate in LPFVT patients [16]. However, some studies have reported that performing ablation at sites distal to the earliest P2 potential can terminate LPFVT but may induce upper septal fascicular ventricular tachycardia [17,18]. When the P1 potential is recorded during the procedure, the optimal ablation target should be the P1 site or the connecting region between P1 and P2. If P1 potentials cannot be identified, the earliest P2 potential should be selected as the primary target [19].
CONCLUSION
Left posterior fascicular ventricular tachycardia is a verapamil-sensitive idiopathic arrhythmia, and its recurrent episodes can result in tachycardia-induced cardiomyopathy. Catheter ablation is the preferred therapeutic strategy. In this case, a retrospective diagnosis of tachycardia-induced cardiomyopathy was established based on the patient’s recurrent ventricular tachycardia, progressive decline in cardiac function, and normalization of cardiac function following a successful radiofrequency ablation.
AUTHOR CONTRIBUTIONS
Feng Xue and TingBo Jiang are guarantors of the study, have full access to all the data in the study, and take responsibility for the data’s integrity and accuracy.
Study concept and design: NingNing Zheng, Yiyuan Chen, YongBing Fu, FangFang Zhang1, Lin Ling Acquisition, analysis, or interpretation of data: All authors.
Drafting the manuscript: NingNing Zheng
Critical revision of the manuscript for important intellectual content: All authors.
Administrative, technical, or material support: All authors.
Study supervision: Feng Xue and TingBo Jiang.
Data availability: The data will be shared upon reasonable requests to the corresponding author.
PATIENT CONSENT STATEMENT
The patient consented to the publication of this study.
How to Cite
References
URL: https://pubmed.ncbi.nlm.nih.gov/7317238/
URL: https://pubmed.ncbi.nlm.nih.gov/16171747/
URL: https://pubmed.ncbi.nlm.nih.gov/37480871/
URL: https://pubmed.ncbi.nlm.nih.gov/32612855/
URL: https://pubmed.ncbi.nlm.nih.gov/39959626/
URL: https://pubmed.ncbi.nlm.nih.gov/31990473/
URL: https://pubmed.ncbi.nlm.nih.gov/1735164/
URL: https://pubmed.ncbi.nlm.nih.gov/31456374/
URL: https://pubmed.ncbi.nlm.nih.gov/28855272/
URL: https://pubmed.ncbi.nlm.nih.gov/30833535/
URL: https://pubmed.ncbi.nlm.nih.gov/24926333/
URL: https://pubmed.ncbi.nlm.nih.gov/29383491/
URL: https://pubmed.ncbi.nlm.nih.gov/19632533/
URL: https://pubmed.ncbi.nlm.nih.gov/34317296/
URL: https://pubmed.ncbi.nlm.nih.gov/27635071/
URL: https://pubmed.ncbi.nlm.nih.gov/29759464/
URL: https://pubmed.ncbi.nlm.nih.gov/28491644/
URL: https://pubmed.ncbi.nlm.nih.gov/31449630/
URL: https://pubmed.ncbi.nlm.nih.gov/27635075/