Abstract
Patent foramen ovale (PFO) is an embryonic defect in the interatrial septum, which has been associated with migraine, high-altitude deoxygenation syndrome, decompression sickness and transient ischemic attacks (TIA) in patients aged 18-65 years. Atrial septal aneurysm (ASA), characterized by a protrusion of the atrial septum, exacerbates the risk of unexplained embolic events in patients with PFO. Therefore, intervention for PFO with ASA is highly recommended.
The tunnel technique is frequently employed to close PFO. However, in patients with ASA, it often results in significant residual atrial septal flutter following occluder implantation. In contrast, the use of a single occluder for simultaneous closure of PFO, ASA and atrial septal defect (ASD) under the transseptal puncture is rarely applied.
Keywords
CASE REPORT
A 37-year-old female was admitted to our hospital with migraine. Preoperative transesophageal echocardiography revealed a PFO and ASA, with the ASA measuring 28.7mm in length and 10.7mm in depth (Figure 1A-C). To our surprise, the patient was also found to have a small ASD located close to the opening of the PFO, measuring 1.73mm in size (Figure 1D, Video 1).
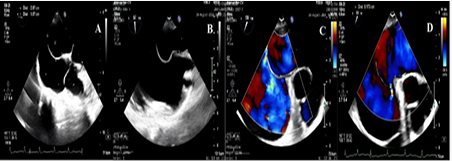
Figure 1: The image of the complex congenital heart disease. (A)The length of ASA is 28.7mm and the depth is 10.7mm. (B-C). The image of PFO at different view. (D)A small ASD located close to the opening of the PFO, measuring 1.73mm in size. The ++ means the distance.
Video 1: Preoperative transesophageal echocardiography.
Furthermore, contrastenhanced transthoracic echocardiography (cTEE) demonstrated a moderate to severe right-to-left shunt (Video 2). It presents a complex scenario of congenital heart disease, necessitating a simultaneous intervention using a single occluder to address all the defects.
Video 2: The result of contrast transthoracic echocardiography
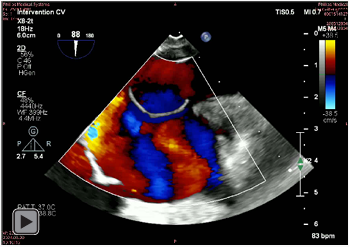
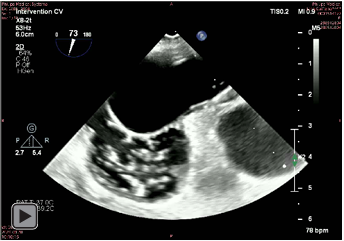
Under general anesthesia, the right femoral vein was punctured. An 8.5F Swartz sheath and Brockenbrough needle were then used to perform an atrial septal puncture under the guide of TEE (Figure 2A-B). The puncture site was carefully selected based on the parallel distance from the PFO orifice to the lowest point of the ASA. Following successful atrial septal puncture, heparin (100 U/kg) was administered intravenously. Based on the puncture side and the anatomical characteristics, a 28/28mm occlude (MenoCarna, Shanghai shape memory Alicy, LEPU Medical, China) was selected and implanted through the delivery sheath (Figure 2C-D, Video 3).
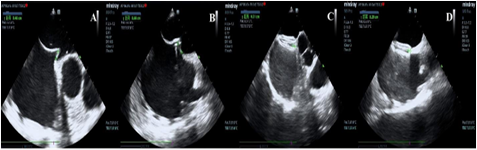
Figure 2: The procedure of patient undergoing precise transseptal puncture technique. (A-B).The distance between the puncture point to the tip of PFO is 4.6mm at aortic short-axis and 6.8mm at bicaval view. (C-D)The length of tissue grasped by the occluder measures 3.1mm at aortic short-axis and 2.9mm at bicaval view. The ++ means the distance.
Video 3: The morphology following the precise transseptal puncture technique.
A follow-up echocardiogram revealed that the occluder was well-seated, with no residual signs of the ASA (Figure 3A-C), and the degree of right-to-left had shunt decreased too mild.

Figure 3: The morphology of the occluders during the follow-up. (A) An obvious ASA before the procedure (B-C). The occluder was well seated, with no residual signs of the ASA after transcatheter treatment. The ++ means the distance
CONCLUSION
The precise atrial septal puncture technique, combined with the simultaneous intervention using a single occluder, not only ensured a technically successful closure of the PFO and ASD, but also nearly resolved the ASA concurrently.
CONSENT STATEMENT
The authors confirm that informed consent was obtained from the patient for the study described in the manuscript and to the publication of their data.