Abstract
Background : Atrial fibrillation (AF) is remarkably common in patients with obstructive hypertrophic cardiomyopathy (oHCM) and is associated with considerable symptoms and poor survival. Studies on the relationship between HRV and AF in patients with HCM are lacking. Herein, we aimed to investigate whether the addition of HRV variables can improve AF detection in these patients.
Methods: We consecutively enrolled 1,112 patients with oHCM, including 158 patients with AF. The HRV variables included the standard deviation of normalto-normal intervals (SDNN), root mean squared successive difference (rMSSD), and percentage of cycles differing from the preceding cycle by >50ms (percentage of normal-to-normal (NN) intervals that differ by more than 50 milliseconds [pNN50]). SDNN, rMSSD, and pNN50 were also transformed into binary variables underlying the cutoff values for AF diagnosis (termed SDNN_cutoff, rMSSD_cutoff, and pNN50_cutoff, respectively).
Results: The mean age of this cohort was 48.94±12.37 years, and 451 (40.6%) patients were female. The SDNN, rMSSD, and pNN50 were higher in patients with AF than in their counterparts. In multivariate analysis, HRV variables were independently associated with AF, and pNN50_cutoff had the largest effect size (odds ratio 7.86) among the HRV variables. Age, body mass index, hyperlipidemia, left atrial diameter, and left ventricular outflow tract gradient were included in the control model for AF diagnosis (area under the curve [AUC] 0.719). Adding HRV variables to the control model separately, the model including pNN50_cutoff performed best in identifying AF among all models (AUC 0.736) and had a significant integrated discrimination improvement (IDI) compared with the control model (IDI=0.064).
Conclusions: HRV was independently associated with AF, and adding HRV variables to the model improved AF detection, particularly pNN50_cutoff.
Keywords
Abbreviations AF
Atrial Fibrillation; oHCM: Obstructive Hypertrophic Cardiomyopathy; HRV: Heart Rate Variability; SDNN: Standard Deviation of Normal-to Normal Intervals; rMMSD: Root Mean Square Difference of Successive Normal-to-Normal Intervals; pNN50: Percentage of Normal-to-Normal Intervals that Differ by More than 50 Milliseconds; AUC: Area under the Curve; IDI: Integrated Discrimination Improvement; HCM: Hypertrophic Cardiomyopathy; ANS: Autonomic Nervous System; LAD: Left Atrial Diameter; RR: R-Wave to R-Wave Interval; LV: Left Ventricular; ROC: Receiver Operating Characteristic; AIC: Akaike Information Criterion; NRI: Net Reclassification Improvement; IDI: Integrated Discrimination Improvement; BMI: Body Mass Index.
INTRODUCTION
Atrial fibrillation (AF) is the most common arrhythmia in hypertrophic cardiomyopathy (HCM), occurring in approximately 20% of patients with HCM [1]. Patients with AF are more likely to experience considerable symptoms and have a worse long-term prognosis [2,3]. Given its high prevalence and morbidity, understanding the mechanisms and detection of AF in patients with HCM is critical for early intervention [4]. Several pathophysiological mechanisms underlying the development of AF have been studied in the general population [5,6]. In recent years, increasing evidence has suggested that autonomic nervous system (ANS) dysfunction, including sympathetic and parasympathetic dysfunction, is involved in the pathogenesis of AF [7,8]. Previous studies have confirmed the presence of ANS dysfunction in patients with HCM [9,10]. However, no association between ANS dysfunction and AF has been reported in patients with HCM.
Heart rate variability (HRV) changes slightly during consecutive cardiac cycles and can be quantified to assess the sympathetic and parasympathetic tones of the cardiac ANS [11]. A twenty-four hour Holter monitor can be used to evaluate HRV and as a noninvasive assessment of the cardiac ANS [12]. HRV has been extensively studied in the general population and has important prognostic implications for various cardiovascular diseases [13-15]. ANS dysfunction is a potential trigger for new-onset AF and a risk factor for AF [16]. However, studies on the relationship between HRV and AF in patients with HCM are lacking. Here, we aimed to investigate the association between HRV and AF in patients with obstructive HCM (oHCM), and whether adding HRV variables can improve the detection of AF.
MATERIALS AND METHODS
Study Population
Between January 2015 and December 2019, 1,491 patients with obstructive HCM who underwent septal myectomy at our institution were scanned. Of the 1,491 patients, 379 were excluded for the following reasons: 1) absence of a preoperative ambulatory Holter electrocardiogram (ECG) evaluation or 24-hour Holter ECG-recorded AF, 2) prior history of heart surgery, and 3) preoperative permanent pacemaker installation. Consequently, 1,112 patients were included in the final analysis. The diagnosis of HCM was based on the American Heart Association and American College of Cardiology guidelines [17], which mainly included unexplained septal hypertrophy with a thickness>15 mm or a septal cardium with a thickness>13 mm, and a family history of HCM in the absence of other cardiac or systemic diseases. Septal myectomies were performed on patients whose symptoms were refractory to drug treatment and who had a left ventricular outflow tract (LVOT) gradient ≥50 mmHg at rest or during provocation. Septal myectomy (extended Morrow procedure) was performed as previously described [18]. All patients signed informed consent forms before enrollment, and the study was approved by the Ethics Committee of Fuwai Hospital. All the procedures were conducted in accordance with the ethical principles of the Declaration of Helsinki.
Twenty-Four-Hour Holter ECG Monitoring
All patients in this study underwent 24-hour Holter ECG monitoring (BI9800; Biomedical Instruments Co., Ltd., Osaka, Japan) 2–5 days before surgery. Sinus rhythm was mandatory for study entry, and each 24-hour Holter required at least 20 h of artifact-free data. Holter recordings were computer-analyzed, and all Holter readings were checked by the investigators. The time-domain analysis of HRV included the standard deviation of normal-to-normal intervals (SDNN), the standard deviation of mean normal to-normal intervals for each 5-minute segment of a 24-hour HRV recording (SDANN), the root mean square difference of successive normal-to-normal intervals (rMMSD), and the percentage of NN50 (normal-to-normal intervals >50 ms) in the total number of R-wave to R-wave (RR) intervals. In the time domain index, SDNN reflects total sympathetic and parasympathetic nervous system activity, whereas SDANN reflects sympathetic nervous system tone. Root mean squared successive difference (RMSSD) reflects changes in the parasympathetic nervous system tone, and the percentage of normal-to-normal (NN) intervals that differ by more than 50 milliseconds (pNN50) reflects the parasympathetic nervous system tone activity.
Echocardiography
Two experienced physicians conducted the echocardiographic examinations using an E9 ultrasound system (General Electric Company, Boston, MA, USA). All patients underwent preoperative and postoperative two dimensional and Doppler echocardiography. Left atrial diameter (LAD), left ventricular (LV) end-diastolic diameter, LV ejection fraction, and ventricular septal thickness were measured according to the recommendations of the American Society of Echocardiography [19]. LVOT gradient was calculated using the simplified Bernoulli equation: These methods are described in detail in our previous publication [18].
AF Diagnosis and Evaluation
The diagnosis of AF met the definition of the 2020 European Society of Cardiology Guidelines [20]: A standard 12-lead ECG recording or a single-lead ECG tracing of ≥30s showing a heart rhythm with no discernible repeating P waves and irregular RR intervals is considered diagnostic of clinical AF. AF was defined as a preoperative diagnosis confirmed by a 12-lead ECG or a documented history before myectomy.
Statistical Analysis
Categorical variables are presented as numbers and percentages, and continuous variables as means and standard deviations or medians with interquartile ranges, as appropriate. Differences in characteristics across groups were compared using analysis of variance or the chi-square test. Correlations between continuous and categorical variables were assessed using Pearson’s or Spearman’s correlation coefficients, as appropriate. Receiver operating characteristic (ROC) curves were constructed to explore the optimal cutoff value of each HRV variable for detecting AF before transforming the HRV variables into categorical variables as candidates for logistic regression analysis models. Univariate and multivariate logistic regression analyses were performed to determine the association between HRV and AF. All relevant clinical and echocardiographic variables were included in the multivariate model, with a p-value<0.1. Multivariate logistic regression models were constructed by adjusting the variables from the univariate analysis using a backward method before adding each HRV variable to the multivariate logistic regression model separately as the final model. The Akaike information criterion (AIC) was used to compare the goodness of fit of each model, and model discrimination was assessed by comparing the area under the curve (AUC), net reclassification improvement (NRI), and integrated discrimination improvement (IDI). A nomogram was constructed based on the optimal model to estimate AF probability. All statistical analyses were performed using the R version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria) and GraphPad Prism version 8.0 (GraphPad Software Inc., La Jolla, CA, USA).
RESULTS
Clinical Characteristics of the Study Cohort
The 1,112 consecutive patients with oHCM included 158 with AF and 954 without AF. The mean age of the study population was 48.94±12.37 years, and 451 (40.6%) patients were female. The baseline characteristics of these patients were grouped into those with and without AF, and the results are summarized in Table 1.
Table 1: Baseline characteristics of the study population
|
Variables |
Overall |
Patient Without AF (N=954) |
Patients with AF (N=158) |
p |
||||
|
Female (N,%) |
451 (40.6) |
394 (41.3) |
57 (36.1) |
0.25 |
||||
|
Age,year |
48.94 (12.37) |
48.35 (12.30) |
52.53 (12.24) |
<0.001 |
||||
|
BMI kg/m2 |
25.60 (3.48) |
25.52 (3.44) |
26.08 (3.68) |
0.065 |
||||
|
Heart rate beats/min |
71.94 (9.74) |
71.92 (9.34) |
72.06 (11.89) |
0.866 |
||||
|
Systole blood pressure (mmHg) |
124.14 (15.35) |
124.45 (15.35) |
122.26 (15.29) |
0.097 |
||||
|
Diastole blood pressure (mmHg) |
72.68 (10.16) |
72.70 (10.01) |
72.54 (11.07) |
0.855 |
||||
|
Chestpain (N,%) |
384 (34.5) |
336 (35.2) |
48 (30.4) |
0.274 |
||||
|
Synscope (N,%) |
253 (22.8) |
216 (22.6) |
37 (23.4) |
0.91 |
||||
|
amaurosis (N,%) |
237 (21.3) |
201 (21.1) |
36 (22.8) |
0.702 |
||||
|
palpitation(N,%) |
306 (27.5) |
231 (24.2) |
75 (47.5) |
<0.001 |
||||
|
Diabetes Mellitus (N,%) |
63 (5.7) |
52 (5.5) |
11 (7.0) |
0.565 |
||||
|
Hyperlipidemia (N,%) |
373 (33.5) |
310 (32.5) |
63 (39.9) |
0.084 |
||||
|
Hypertesion (N,%) |
337 (30.3) |
285 (29.9) |
52 (32.9) |
0.499 |
||||
|
Coronary artery disease (N,%) |
156 (14.0) |
137 (14.4) |
19 (12.0) |
0.51 |
||||
|
Previous heart surgery (N,%) |
76 (6.8) |
61 (6.4) |
15 (9.5) |
0.208 |
||||
|
NYHA III/IV (N,%) |
855 (76.9) |
734 (76.9) |
121 (76.6) |
1 |
||||
|
Echocardiographic parameters |
||||||||
|
Left atrial diameter (mm) |
45.09 (6.71) |
44.49 (6.46) |
48.69 (7.09) |
<0.001 |
||||
|
IVST (mm) |
19.99 (5.02) |
20.01 (5.03) |
19.84 (4.93) |
0.683 |
||||
|
LVEDD (mm) |
42.88 (5.03) |
42.82 (4.97) |
43.26 (5.40) |
0.304 |
||||
|
LVEF (%) |
69.45 (5.48) |
69.52 (5.57) |
69.05 (4.91) |
0.317 |
||||
|
RVD (mm) |
21.39 (3.00) |
21.33 (3.02) |
21.74 (2.85) |
0.114 |
||||
|
MLVWT(mm) |
22.21 (4.83) |
22.30 (4.96) |
21.68 (3.97) |
0.14 |
||||
|
Gradient (mmHg) |
83.51 (29.46) |
84.80 (29.38) |
75.77 (28.89) |
<0.001 |
||||
|
Moderate or severe MR (N,%) |
589 (53.0) |
502 (52.6) |
87 (55.1) |
0.629 |
||||
|
Medical therapy |
||||||||
|
β receptor blocker (N,%) |
1064 (95.7) |
910 (95.4) |
154 (97.5) |
0.327 |
||||
|
Calcium channel blocker (N,%) |
360 (32.4) |
304 (31.9) |
56 (35.4) |
0.425 |
||||
|
HRV |
||||||||
|
SDNN (ms) |
114.13 (47.61) |
112.35 (45.00) |
124.89 (60.15) |
0.002 |
||||
|
SDANN (ms) |
100.65 (66.18) |
100.12 (63.54) |
103.92 (80.56) |
0.507 |
||||
|
rMSSD (ms) |
34.51 (28.11) |
32.96 (27.96) |
43.90 (27.21) |
<0.001 |
||||
|
pNN50 (%) |
12.04 (14.24) |
10.75 (11.95) |
19.91 (22.33) |
<0.001 |
||||
Compared to patients without AF, the patients with AF were older (52.53±12.24 vs. 48.35±12.30 years, p<0.01), more likely to have palpitation (47.5% vs. 24.2%, p<0.01), had a larger LAD (48.69±7.09 vs. 44.49±6.46 mm, p<0.01), and had a lower LVOT gradient (75.77±28.89 vs. 84.80±28.89 mmHg, p<0.01). Moreover, SDNN (124.89±60.15 vs. 112.35±45.00, p=0.002), rMSSD (43.90±27.21 vs. 32.96±27.96, p<0.01), and pNN50 (19.91±22.33 vs. 10.75±11.95, p<0.01) were significantly increased in patients with AF compared to those without AF. Values are expressed as the mean ± standard deviation or median (range) or number (percentage). BMI: body mass index, NYHA: New York Heart Association, IVST: interventricular septal thickness, LVEDD: left ventricular end-diastolic diameter, RVD: right ventricular diameter, LVEF: left ventricular ejection fraction, LVEF: left ventricular ejection fraction, MLVWT: maximal left ventricular wall thickness, MR: mitral regurgitation. SDNN, the standard deviation of the mean R-R intervals; SDANN, the standard deviation of mean normal-to-normal intervals for each 5-minute segment of a 24-hour HRV recording; rMSSD, root mean squared successive difference; pNN50, percentage of cycles differing from the preceding one by > 50 ms. Significant p-values (p < 0.05) are presented in bold.
The other clinical variables listed in Table 1 were comparable between the two groups.
Correlation Analysis Between HRV and Clinical Parameters
We analyzed the correlation between the time-domain metrics of HRV and clinical data, and the results are summarized in Supplementary Figure 1. The LAD was positively correlated with rMSSD (r=0.09, p<0.01) and pNN50 (r=0.089, p<0.01). The preoperative LVOT gradients were negatively correlated with rMSSD (r=–0.10, p<0.01) and pNN50 (r=–0.11, p<0.01), whereas PNN50 was strongly correlated with rMSSD (r=0.96, p<0.01) and SDNN (r=0.48, p<0.01).
Logistic Regression Analyses of Risk Factors for AF Episodes
Before the univariate analysis, we plotted ROC curves to determine the optimal cutoff values of HRV variables for the diagnosis of AF and then transformed the HRV variables into categorical variables underlying the cutoff value, which were termed SDNN_cutoff, rMSSD_cutoff, and pNN50_cutoff. The results of the ROC curves are presented in Supplementary Figure 2, and the cutoff values for SDNN, rMSSD, and PNN50 were 153.5, 34.5, and 43.5, respectively. The results of the univariate logistic regression analysis are summarized in Supplementary Table 1. Age, body mass index (BMI), hyperlipidemia, LAD, and LVOT gradient were included in the multivariate regression analysis to construct the control model. The HRV variables were then added separately to the control model to construct new models. The results of the multivariate logistic regression analysis for AF are presented in Table 2.
Table 2: Multivariable logistic regression analysis models for AF
|
Variables |
Crude OR |
95%CI |
p |
Adjusted OR |
95%CI |
p |
|
SDNN |
1.00 |
1.00- 1.01 |
0.006 |
1.004 |
1001 - |
<0.001 |
|
1.01 |
||||||
|
SDNN_cutoff |
2.11 |
1.37-3.20 |
<0.001 |
2.26 |
1.41-3.57 |
<0.001 |
|
rMSSD |
1.01 |
1.01 - 1.02 |
<0.001 |
1.01 |
1.003 - |
0.010 |
|
1.02 |
||||||
|
rMSSD_cutof |
2.14 |
1.52-3.01 |
<0.001 |
2.09 |
1.45-3.01 |
<0.001 |
|
f |
||||||
|
pNN50 |
1.03 |
1.02 - 1.04 |
<0.001 |
1.03 |
1.02 - 1.04 |
<0.001 |
|
pNN50_cutof |
9.90 |
5.67-17.51 |
<0.001 |
7.86 |
4.25-14.7 |
<0.001 |
|
f |
SDNN indicates the standard deviation of the mean R-R intervals; rMSSD, root mean squared successive difference; pNN50, percentage of cycles differing from the preceding one by > 50 ms. The SDNN, rMSSD, and pNN50 were transformed into binary variables underlying the cutoff for AF detection termed SDNN_cutoff, rMSSD_cutoff, and pNN50_cutoff, respectively. OR, odds ratio, CI, confidential interval. Each model has adjusted for age, body mass index, hyperlipidemia, left atrial diameter and left ventricular outflow tract gradient
After adjusting for age, BMI, hyperlipidemia, LAD, and LVOT gradients, we observed that SDNN, rMSSD, and pNN50 were independently associated with a higher prevalence of AF. Additionally, SDNN_cutoff, rMSSD_cutoff, and pNN50_cutoff were independent indicators of AF. Among these variables, pNN50_cutoff had the largest effect size, with an odds ratio of 7.86 (95% confidence interval [CI]: 4.25–14.7).
Assessing the Performance of HRV Models for AF Detection
As described earlier, we added HRV variables separately to the control model to construct new models and then evaluated the performance of each new model. The results are summarized in Table 3.
Table 3: Performance of SDNN, rMSSD, and pNN50 for detecting atrial fibrillation
|
Variables |
AUC |
P |
NRI |
P |
IDI |
P |
AIC |
|
(95%CI) |
(95%CI) |
(95%CI) |
|||||
|
Control |
0.719 |
- |
- |
- |
- |
- |
813.7 |
|
(0.673-0.765) |
|||||||
|
SDNN (vs.control) |
0.725 |
0.36 |
0.264 |
0.002 |
0.015 |
0.006 |
804.8 |
|
(0.679-0.770) |
7 |
(0.094-0.434) |
(0.004-0.026) |
||||
|
0.731 |
0.23 |
0.250 |
0.041 |
<0.00 |
|||
|
rMSSD (vs.control) |
(0.687-0.776) |
2 |
(0.083-0.417) |
0.003 |
(0.022-0.061) |
1 |
787.5 |
|
0.729 |
0.36 |
0.238 |
0.048 |
<0.00 |
|||
|
pNN50 (vs.control) |
(0.684-0.774) |
7 |
(0.073-0.404) |
0.004 |
(0.026-0.070) |
1 |
784.0 |
|
SDNN_cutoff |
0.721 |
0.74 |
0.053 |
0.016 |
|||
|
(vs.control) |
(0.675-0.767) |
2 |
(-0.004-0.109) |
0.070 |
(0.006-0.026) |
0.002 |
804.6 |
|
rMSSD_cutoff |
0.732 |
0.19 |
0.070 |
0.018 |
<0.00 |
||
|
(vs.control) |
(0.687-0.776) |
5 |
(0.010-0.130) |
0.022 |
(0.008-0.030) |
1 |
800.1 |
|
pNN50_cutoff |
0.736 |
0.06 |
0.149 |
<0.00 |
0.064 |
<0.00 |
774.0 |
|
(vs.control) |
(0.690-0.782) |
3 |
(0.074-0.225) |
1 |
(0.037-0.091) |
1 |
AUC indicates area under the curve; NRI, net reclassification improvement; IDI, integrated discrimination improvement; AIC, Akaike information criterion. Control model means the multivariable logistic model contained variables from univariable analysis after adjusting using a backward method, in which including age, body mass index, hyperlipidemia, left atrial diameter, and left ventricular outflow tract gradient. other abbreviations can be found in table2
The difference in AUC between the new and control models was not significant; however, the NRI and IDI in the new models improved significantly. The model including pNN50_cutoff had the largest AUC (0.736; 95% CI: 0.690–0.782), highest IDI (0.064), and lowest AIC (774), indicating the best fit compared with the other models. A nomogram was developed based on the new pNN50_cutoff model to calculate the probability of AF (Figure 1A), which included age, BMI, hyperlipidemia, LAD, LVOT gradient, and pNN50_cutoff. The calibration curve for the nomogram was close to the 45° diagonal for the most part; however, it slightly exceeded the diagonal at a high predicted risk, indicating that the nomogram was well calibrated in most situations. In contrast, it might underestimate the risk when the risk is already high (Figure 1B). The AUC of the new model of the pNN50_cutoff was 0.736 (95% CI: 0.690-0.782), demonstrating good discriminative ability of the model (Figure 1C).
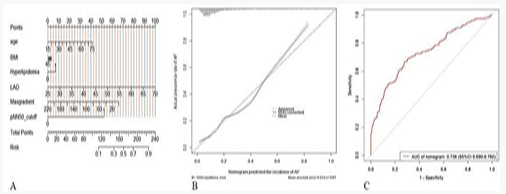
Figure 1A: the nomogram was developed based on the pNN50 cutoff model to calculate the probability of AF detection, and the model included age, BMI, hyperlipidemia, LAD, LVOT gradient and pNN50_cutoff; 1B, the calibration curve for the nomogram was mostly close to the 45° diagonal but slightly exceeded the diagonal at high predicted risk; 1C, the AUC of nomogram.
We further divided the SDNN, rMSSD, and pNN50 into five groups according to their quintile intervals and investigated the prevalence of AF in each group, including the prevalence of AF in patients having less than and more than the cut-off values of the SDNN, rMSSD, and pNN50. A positive Spearman’s linear association was observed between AF prevalence and SDNN (Figure 2A), rMSSD (Figure 2) (Figure 2B), and pNN50 (Figure 2C). The prevalence of AF in patients with SDNN>153.5 or rMSSD>34.5 (cutoff value) was 23.5% and 20.5%, respectively, nearly two-fold higher than that in their counterparts. Notably, we observed that the prevalence of AF in patients with pNN50>43.5 was 57.1%, five-fold higher than that in their counterparts, suggesting that pNN50 is a good indicator of AF with high specificity in patients with oHCM.

Figure 2: A positive Spearman’s linear association was observed between the prevalence of AF and SDNN (Figure 2A), rMSSD (Fig ure 2B), and pNN50 (Figure 2C). The prevalence of AF in patients with SDNN > 153.5 or rMSSD > 34.5 (cutoff value) was 23.5% and 20.5%, respectively, the prevalence of AF in patients with pNN50 > 43.5 was 57.1%.
DISCUSSION
The findings of the current study can be summarized as follows: HRV variables were significantly higher in patients with AF than in those without AF. SDNN, rMMSD, and pNN50 were independently associated with a higher prevalence of AF, and positive Spearman’s linear associations were observed between the prevalence of AF and SDNN, rMMSD, and pNN50. Furthermore, in multivariable models, the model including pNN50_cutoff had the largest effect size, with an odds ratio of 7.86 (95% CI: 4.25-14.7) for AF detection, while it had the largest AUC (0.736; 95% CI: 0.690–0.782), the highest IDI (0.064), and the lowest AIC (774), indicating that the addition of HRV variables can improve the diagnostic ability of AF in patients with oHCM, particularly pNN50_ cutoff.
The cardiac ANS contains both extrinsic and intrinsic cardiac ANSs, including the sympathetic and parasympathetic nervous systems. The parasympathetic nervous system includes the epicardial autonomic ganglia, fat pad, and the associated connecting nerve fibers, which form a broad and highly connected epicardial neural network [21]. When activated, different physiological effects occur to maintain stable balance and sinus rhythm in the heart. It can be induced or promoted when the ANS is imbalanced [22]. In clinical practice, directly monitoring autonomic nerve activity is challenging, and cardiac autonomic regulation and remodeling can only be indirectly evaluated. Therefore, considering the specificity and sensitivity of clinical surveillance, the selection of HRV parameters on a 24 h Holter monitor to reflect cardiac ANS activity is currently the primary research approach [12]. HRV describes the oscillations between the RR intervals of a continuous heartbeat in Holter monitoring, which can be viewed as periodic changes in heart rhythm over time and constitutes a noninvasive method for the qualitative and quantitative evaluation of the ANS.
In this study, we analyzed the overall HRV profiles of patients with HCM using a large dataset. Our results demonstrated that the overall HRV of patients with HCM was decreased compared to the normal values of each index, indicating that ANS activity was reduced in patients with HCM. This is similar to the results of previous studies, most of which revealed that autonomic dysfunction in patients with HCM was dominated by decreased parasympathetic nervous system activity and increased sympathetic nervous system activity [23,24]. Autonomic dysfunction, represented by reduced HRV, is a risk factor for poor prognosis in cardiovascular diseases, such as ventricular arrhythmias and sudden death [25]. However, to the best of our knowledge, no previous study has conducted HRV analysis of AF in patients with HCM.
AF occurs via various mechanisms, including electrical, structural, and neural remodeling, inflammation, and oxidative stress [5,6]. The cardiac ANS plays a substantial role in the development of AF [7]. We demonstrated that SDNN (representing total autonomic activity), RMSSD, and PNN50 (representing parasympathetic activity) were significantly increased in patients with HCM who developed AF compared to those who did not, suggesting that total ANS activity and parasympathetic nervous system activity are increased in patients with HCM. We speculate that patients with HCM who have experienced AF have increased autonomic activity, predominantly based on increased parasympathetic activity, including the original ANS tone, which is of great significance in developing and maintaining AF [26]. Acetylcholine released in the physiological state of the parasympathetic nerves binds to the M2 receptors on cardiomyocytes, causing a decrease in rhythm, conduction, and myocardial contractility, thereby inhibiting cardiac activity. Thus, parasympathetic nerves weaken the heart under normal conditions [27]. Smeets et al. [28], demonstrated that moderate stimulation of the parasympathetic nervous system shortens the impulse length and decreases the size of re-entrant circuits, contributing to AF. Moreover, Schauerte et al. [29], reduced the effective refractory period at various atrial sites by stimulating the bilateral cervical vagus nerves, thereby triggering AF. This evidence suggests that ANS activation can trigger AF by causing changes in atrial electrophysiology through acetylcholine release via nerve endings. AF also interferes with the distribution and function of the vagus nerve in the atria, which increases vagus tension and stabilizes the AF. A recent Mendelian randomization study [30], confirmed a significant correlation between HRV measurements and new-onset AF in the general population, supporting a causal relationship between the two. Furthermore, Fioranelli et al. [31], observed a decrease in the left frequency (LF), LF/high frequency (HF) ratios, and an increase in the HF ratio in patients with paroxysmal AF without structural heart disease, suggesting an elevated vagal tone, which is consistent with our findings.
Our results demonstrated that SDNN, rMSSD, and pNN50 all correlated with the occurrence of AF in patients with HCM and were independent indicators of AF. Moreover, adding each of the three variables to the multivariate model improved the diagnostic ability of AF, particularly pNN50 and rMSSD, further confirming the relationship between changes in parasympathetic tone and AF occurrence in patients with HCM. This is similar to the finding that rMSSD and PNN50 are independent risk factors for AF recurrence after radiofrequency ablation, in which parasympathetic nerves are believed to play a key role [16]. The results of a recent meta-analysis of HRV similarly confirmed previous findings [32], in that the higher the SDNN and rMSSD, the more imbalanced the autonomic regulation and predominance of parasympathetic regulation, and the more easily AF is maintained. Sympathetic excitation is associated with the development of ventricular arrhythmias [33], and when sympathetic excitability is relatively enhanced, myocardial electrical stability is diminished, which predisposes individuals to malignant ventricular arrhythmias. In contrast, our results demonstrate that increased parasympathetic activity is associated with the development of AF in patients with HCM.
We also observed a negative correlation between SDNN and both age (p<0.01) and BMI (p< 0.01), suggesting that the total autonomic tone activity decreases with age and BMI. Our previous study demonstrated that age and BMI were independent risk factors for perioperative AF in patients with HCM [34], suggesting that HRV may play a role in the development of AF through age and BMI. Moreover, LAD positively correlated with rMSSD (p<0.01) and pNN50 (p<0.01). However, the correlation between left atrial size and AF has been widely verified [35], suggesting that changes in the parasympathetic nervous system tension may be associated with the occurrence of AF through changes in left atrial size. Furthermore, the preoperative LVOT gradient was negatively correlated with rMSSD (r=–0.10, p<0.01) and pNN50 (r=–0.11, p<0.01), which suggests that for patients with HCM, the higher the LVOT gradient, the lower the parasympathetic tone, and the less prone they are to AF. AF is less likely to occur in patients with oHCM [36]. Our study provides an alternative explanation for these results by showing that the LVOT gradient in patients with HCM may influence the parasympathetic tone, which in turn influences AF occurrence.
Some studies [32,37], have reported ANS changes before and after paroxysmal AF episodes, with findings suggesting that sympathetic and parasympathetic imbalance play an important role in AF episodes; however, we did not analyze HRV before and after AF episodes in 24 h Holter results. Prolonged HRV measurements (24 h) are more appropriate for estimating an individual’s basal autonomic state. Short-term (5 min) HRV measurements provide information about the system dynamics that disrupt basal homeostasis and may be part of the trigger for arrhythmias, as well as atrial or ventricular premature beats [38].
Our study had some limitations. First, the diagnosis of AF in our study was based on 12-lead ECG and previous medical records, which may have missed some patients who had AF episodes, did not undergo electrocardiography, or were not mentioned in the medical records. Second, for technical reasons, excluding patients with multiple premature atrial beats during the ambulatory ECG recording period was necessary, which may have been the target population for our study. Third, because this study was retrospective, no causal conclusions could be drawn. Fourth, some patients received medication during the 24 h Holter recording period, which may have affected the HRV measurements. However, at baseline, the proportion of medications used by patients with and without AF did not differ significantly, suggesting that the medication itself may have no significant effect. HRV is an indirect measure of cardiac autonomic tone; therefore, the results of the present study should be interpreted with caution.
CONCLUSIONS
HRV was significantly higher in patients with oHCM and AF than in those without AF. SDNN, rMMSD, and pNN50 were independently associated with a higher prevalence of AF, and positive Spearman’s linear associations were observed between the prevalence of AF and SDNN, rMMSD, and pNN50. The addition of HRV variables can improve the diagnostic ability of AF in patients with oHCM, particularly pNN50_cutoff.
AVAILABILITY OF DATA AND MATERIALS
The datasets generated and/or analysed during the current study are not publicly available due to the privacy policy but are available from the corresponding author on reasonable request.
AUTHOR CONTRIBUTIONS
Zhengyang Lu and Changrong Nie contribute for the study design, data analysis and writing the paper. Jiashu Sun, Changsheng Zhu, Tao Lu and Qiulan Yang contribute for data collection. Shuiyun Wang and Yanhai Meng contribute for study concept and revising the paper. All authors read and approved the final manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study complied with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Fuwai Hospital (2023-2048). All patients provided written informed consent.
ACKNOWLEDGMENT
The authors’ deepest gratitude goes to the Information Center of Fuwai hospital for providing us data collection of this study.
FUNDING
This work was supported by grants from (1) Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD0504500), (2) the National Natural Science Foundation of China (Grant No.82570466), (3) Chinese Academy of Medical Sciences (CAMS) Innovation Fund for Medical Sciences (2023-I2M-1-001), and (4) CAMS Innovation Fund for Medical Sciences (2024-I2M-C&T-B-046).
How to Cite
References
URL: https://pubmed.ncbi.nlm.nih.gov/34780764/https:/pubmed.ncbi.nlm.nih.gov/28916640/
URL: https://pubmed.ncbi.nlm.nih.gov/34780764/https:/pubmed.ncbi.nlm.nih.gov/28916640/
URL: https://pubmed.ncbi.nlm.nih.gov/37340493/
URL: https://pubmed.ncbi.nlm.nih.gov/32950468/
URL: https://www.nejm.org/doi/full/10.1056/NEJMcp2023658
URL: https://pubmed.ncbi.nlm.nih.gov/32273035/
URL: https://pubmed.ncbi.nlm.nih.gov/33516396/
URL: https://pubmed.ncbi.nlm.nih.gov/20487120/
URL: https://pubmed.ncbi.nlm.nih.gov/15725307/
URL: https://pubmed.ncbi.nlm.nih.gov/9440705/
URL: https://pubmed.ncbi.nlm.nih.gov/33390146/
URL: https://pubmed.ncbi.nlm.nih.gov/33198486/
URL: https://pubmed.ncbi.nlm.nih.gov/32178902/
URL: https://pubmed.ncbi.nlm.nih.gov/35189879/
URL: https://pubmed.ncbi.nlm.nih.gov/10982537/
URL: https://pubmed.ncbi.nlm.nih.gov/35193492/
URL: https://pubmed.ncbi.nlm.nih.gov/33215931/
URL: https://pubmed.ncbi.nlm.nih.gov/27033027/
URL: https://pubmed.ncbi.nlm.nih.gov/16376782/
URL: https://pubmed.ncbi.nlm.nih.gov/32860505/
URL: https://pubmed.ncbi.nlm.nih.gov/33928710/
URL: https://pubmed.ncbi.nlm.nih.gov/33024501/
URL: https://pubmed.ncbi.nlm.nih.gov/37293795/
URL: https://pubmed.ncbi.nlm.nih.gov/16569542/
URL: https://pubmed.ncbi.nlm.nih.gov/12939209/
URL: https://pubmed.ncbi.nlm.nih.gov/31560809/
URL: https://pubmed.ncbi.nlm.nih.gov/37086229/
URL: https://pubmed.ncbi.nlm.nih.gov/3943157/
URL: https://pubmed.ncbi.nlm.nih.gov/11094046/
URL: https://pubmed.ncbi.nlm.nih.gov/35962833/
URL: https://pubmed.ncbi.nlm.nih.gov/10353133/
URL: https://www.frontiersin.org/journals/cardiovascular-medicine/articles/10.3389/fcvm.2022.1048398/full
URL: https://pubmed.ncbi.nlm.nih.gov/33755139/
URL: https://pubmed.ncbi.nlm.nih.gov/35043680/
URL: https://pubmed.ncbi.nlm.nih.gov/34082914/
URL: https://pubmed.ncbi.nlm.nih.gov/26239580/
URL: https://pubmed.ncbi.nlm.nih.gov/12875412/
URL: https://pubmed.ncbi.nlm.nih.gov/36803313/