Abstract
Congenital aortic-right atrial channel (ARAT) is a very rare congenital cardiovascular malformation characterized by an abnormal channel connection between the aorta and the right atrium [1]. Patients with ARAT are often complicated with other congenital heart malformations and require diagnosis through a variety of imaging examinations. We report a successful diagnosis of ARAT complicated with atrial septal defect and patent ductus arteriosus in a one-month-old baby using low-dose multislice spiral CT (MSCT) due to unclear echocardiography.
Keywords
INTRODUCTION
Aorta-right atrial tunnel (ARAT) is a rare congenital cardiovascular malformation first described by Coto et al. [2], in 1980. It is characterized by an abnormal blood vessel from the descending aorta connected to the right atrium, forming an abnormal left-to-right shunt channel. ARAT can exist alone or be associated with other congenital heart malformations. Due to the left-to-right shunt caused by the deformity which increases pulmonary blood flow and pulmonary artery pressure, patients often show symptoms such as dyspnea, cyanosis, heart failure, and even complications including infective endocarditis or embolism. Therefore, early diagnosis and surgical treatment of the disease is very important.
Several imaging methods can be used for preoperative diagnosis of ARAT. Echocardiography is the most commonly used method for ARAT diagnosis. However, it has limitations in accurately showing the location and shape of abnormal channels, especially when other complex malformations are combined. Magnetic resonance imaging (MRI) is a better diagnostic method for abnormalities of the heart and major blood vessels, but for children, sedation is required during the examination and the process is relatively time-consuming. By contrast, multi-slice CT (MSCT) offers fast scanning speed, high resolution, 3D reconstruction and various post processing methods, making it superior to echocardiography and MRI in displaying the start and end point, direction, and surrounding anatomical structure of abnormal channels.
We report a rare case of a one-month-old girl with an ARAT, along with an atrial septal defect and a patent ductus arteriosus. The ARAT malformation was initially undiagnosed by echocardiography, highlighting the benefits of utilizing low dose MSCT for diagnosing vascular malformations in children.
CASE PRESENTATION
A one-month-old baby girl weighing 5.5kg was admitted to our hospital for treatment because of moaning, spitting, and dyspnea. The parents had no special family history of hypertension and congenital heart disease, and the mother had no special history during pregnancy. Physical examination showed body temperature 36.4, respiratory rate 56 beats/min, heart rate 177 beats/min, blue lips, cyanosis of lips, positive triple concave sign, and systolic murmur of grade 6 in the third intercostal space of the right margin of the sternum during cardiac auscultation.
Echocardiography reported partial anomalous pulmonary venous drainage, patent foramen ovale, pulmonary hypertension, and atrial septal defect. Subsequently, the child was examined by low-dose cardiac CT to better determine the cause of the symptoms. Low-dose CT was performed and showed an abnormal vascular structure starting from the left wall of the ascending aorta and connecting the right atrium, with a maximum diameter of about 10 mm and a length of about 33 mm [Figure A]. CT reformatted images also clearly showed this abnormal channel complicated with patent ductus arteriosus [Figure B] and atrial septal defect [Figure C], and with the significantly dilated pulmonary artery system and hypertrophic right ventricle [Figure C].

[Figure A]:Maximum intensity projection (MIP) showed an abnormal vascular structure starting from the left wall of the ascending aorta and connecting the right atrium, with a maximum diameter of about 10 mm and a length of about 33 mm

[Figure B]:complicated with patent ductus
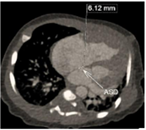
[Figure C]: atrial septal defect and hypertrophic right ventricle
Comprehensive diagnosis of complex congenital heart disease included aortic-right atrial channel, atrial septal defect, patent ductus arteriosus, and pulmonary hypertension. After consultation, a cardiac surgery repair was decided. After the operation, the three abnormal cardiac passages were successfully closed; the diastolic and systolic functions returned to normal; the symptoms of dyspnea disappeared; and only mild tricuspid regurgitation occurred. During the three-month follow-up after the operation, the patient returned to health.
DISCUSSION
ARAT is a rare congenital cardiac vascular malformation of unknown cause characterized by an abnormal channel connection between the aorta and the right atrium [1]. Gajjar et al. [3], suggested that it may be attributed to the abnormal development of elastic fibers in the aortic media and the weakening of support, and the vascular wall gradually expands to a tube under the pressure of the aorta, communicating with the adjacent low-pressure right atrium. Low-dose MSCT is the efficient method to show the ARAT and complicated malformations. In this case, MSCT confirmed the existence of three left-to-right shunt channels (artery-right atrial channel, patent ductus arteriosus channel, and atrial septal defect channel) and confirmed by cardiac surgery. Preoperative CT also plays an important role to display the relationship between the aortic-right atrial channel and coronary artery in planning the patient’s treatment strategy [4].
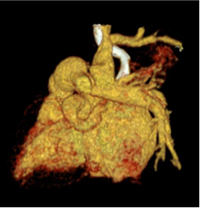
The three left-to-right shunts simultaneously occurs in one patient is a very rare condition which can easily cause pulmonary hypertension, pulmonary infection, Eisenmenger syndrome, right heart failure, and infective endocarditis. Surgery repair should be performed as soon as possible to correct the left-to-right shunt. At present, echocardiography is commonly the first choice for diagnosing congenital heart disease in children, which has the advantages of being non-invasive, economical, and not harmful due to free of radiation. However, accurately assessing ARAT can be challenging due to factors such as difficulties in cooperation, the unique and complex blood flow characteristics, and technical variations among ultrasound operators. For instance, in this scenario, low-dose MSCT showed additional channels between the right atrium and the aorta that were not detectable through echocardiography. Furthermore, the low-dose MSCT images displayed more intuitive information about the abnormal vascular shape and surrounding structures, and the post-processed images clearly highlighted the abnormal structures [Figure D & E].

[Figure D & E]: Volume rendering clearly highlighted the aorta-right atrial tunnel (curved arrow) and its anatomical relationships.
Moreover, MSCT can be scanned in a few seconds and can be synchronized with breathing and heart rate. The powerful post processing techniques can clearly show the complex deformities. However, MSCT examination also has certain limitations, such as the requirement for contrast media injection, radiation exposure that may be disadvantageous for infants and young children. Therefore, when scanning infants and young children using MSCT, we should try to use low dose scanning technology to reduce the radiation dose.
CONCLUSIONS
Congenital aortic-right atrial channel simultaneously complicated with patent ductus arteriosus and ventricular septal defect is a very uncommon condition which easily causes seriously pulmonary hypertension. Low-dose MSCT is superior to ultrasound and MRI for showing extracardiac vascular malformations because of volumetric scanning and multiple post-processing technology. Early diagnosis and early operation benefits patients by avoiding pulmonary hypertension and other complications.
FUNDING
The present study was funded by the Guizhou Provincial Senior Innovative Talent Project (QKHPTRC-GCC [2022]041-1) and Guizhou International Science & Technology Cooperation Base of Precision Imaging for Diagnosis and Treatment (QKT[2024]18).
How to Cite
References
URL: https://www.frontiersin.org/journals/pediatrics/articles/10.3389/fped.2020.00524/full
URL: https://www.sciencedirect.com/science/article/pii/S0022522319377025
URL: https://pubmed.ncbi.nlm.nih.gov/16256780/
URL: https://pubmed.ncbi.nlm.nih.gov/35444840/