Abstract
Background: Ventricular arrhythmia (VA) spectrum ranges from Premature Ventricular contraction (PVC) to Ventricular tachycardia or Ventricular Fibrillation. Depending on etiology and underlying heart disease this may prove to be a life threatening arrhythmia or may have a benign course. Though AAD or ICD is effective, ablation therapy may be adjunctive in certain cases eg VT associated with ischemic heart disease or potentially curative in idiopathic VTs in structurally normal heart. Understanding the mechanism of VT is essential in planning and wisely selecting ablation strategy.
Objective: To review different types of ventricular arrhythmia and understand the pathophysiology, evaluate current technique with brief overview of novel ablation techniques, complications, outcomes of catheter ablation of VT
Methods: This review article summarizes findings from recent clinical trials, text-book chapters, current professional society guideline recommendations.
Conclusion: Advancement in 3D electroanatomic mapping, catheter ablation technology makes VT ablation a safer, feasible effective treatment strategy in carefully selected patient populations.
Abbreviations
ACC: American College of Cardiology; AHA: American Heart Association; ARVC: Arrhythmogenic right ventricular cardiomyopathy; HRS: Heart Rhythm Society; CAD: Coronary Artery Disease; cAMP: Cyclic adenosine monophosphate; CHF: Congestive Heart Failure; CSD: Cardiac Sympathetic Denervation; DAD: Delayed after depolarization; ICD: Implantable Cardioverter Defibrillator; LAD: Left anterior Descending; LBBB: Left bundle branch block; LCC: Left Coronary Cusp; LCSD: Left Cardiac Sympathetic Denervation; LCx: Left Circumflex
LVOT: Left Ventricular Outflow tract; LQTS: Long QT Syndrome; PFA: Pulsed Field Ablation; PVC: Premature Ventricular Contraction; RCC: Right Coronary Cusp; RF: Radio Frequency; RFA: Radio Frequency Ablation
RVOT: Right Ventricular Outflow Tract; SBRT: Stereotactic Body Radiation Therapy; SHD: Structural Heart Disease
STAR: Stereotactic Arrhythmia Radioablation; TdP: Torsades De Pointe; VA: Ventricular Arrhythmia; VT: Ventricular Tachycardia; VF: Ventricular Fibrillation
Keywords
INTRODUCTION
Ventricular arrhythmia spectrum ranges from Premature Ventricular contraction (PVC) to Ventricular tachycardia or Ventricular Fibrillation. Clinical severity may vary from sudden cardiac death to relatively benign idiopathic outflow tract VT seen in structurally normal heart. Whereas catheter ablation is effective and potentially curative in some of these arrhythmias, other forms of VA seen in patients with underlying heart disease may need antiarrhythmic and ICD implantation for secondary prevention. Risk of death is influenced by underlying ischemic heart disease, arrhythmogenic non ischemic cardiomyopathy (e.g. Sarcoidosis, Arrhythmogenic right ventricular cardiomyopathy etc), genetic conditions (e.g. Brugada syndrome, Long QT syndrome etc). In this chapter we will discuss various etiology and electrophysiological mechanisms of VA and role of catheter ablation with the type of VA.
VT is defined as Cardiac arrhythmia [1] of ≥3 consecutive complexes originating in the ventricles at a rate >100 bpm (cycle length: 30 s or needs termination due to hemodynamic compromise in < 30 s, otherwise it is called non sustained VT. It may be monomorphic or polymorphic if there is beat to beat variation in morphology of the QRS complex. Bidirectional VT with a beat-to-beat alternation in the QRS frontal plane axis, often seen in the setting of digitalis toxicity, catecholaminergic polymorphic VT or LQT 7 (Anderson Tawil syndrome). Torsade De Pointe is an example of Polymorphic VT that is typically described in a setting of prolonged QT interval, often initiated by a long short sequence, QRS axis oscillating around the baseline (aptly referring to English translation of French phrase Torsade de pointe to twisting of the point), can be drug induced, or may be seen in extreme bradycardia related to high grade AV block. VF is unorganized rapid chaotic electrical activity with heart rate >300 bpm. This is often a rhythm hemodynamically not tolerated and manifest as syncope followed by quick progression into sudden cardiac arrest/death if not treated promptly.
Etiology and Electrophysiological mechanism of Ventricular arrhythmia
Understanding and identification with accurate diagnosis of VA is imperative to determine ablation target and therapy, and prognostication. Table 1 is not exhaustive but broadly includes types of VA commonly encountered in clinical practice.
Table 1: Different types of Ventricular arrhythmia and their mechanism
|
VA |
Mechanism |
Comment |
|
Idiopathic Outflow tract VT |
Triggered: Catecholamine induced cAMP mediated DAD |
May originate from RVOT or LVOT Responsive to catheter ablation |
|
Scar related post MI VT |
Macro reentrant |
Ischemic heart disease, post MI, CAD |
|
Bundle Branch Reentrant VT |
Macro reentrant |
Dilated cardiomyopathy with infrahisian conduction disease |
|
Fascicular VT |
Reentrant |
Idiopathic, usually benign clinical course |
|
Papillary muscle PVC/VT Mitral/Tricuspid annular PVC/VT |
Focal (triggered activity, triggered activity) |
Exit from left posterior (common) or left anterior papillary muscle |
Idiopathic Outflow tract Ventricular tachycardia
Idiopathic Outflow tract VT is often seen in structurally normal heart. Absence of heart disease is usually suggested by normal ECG (except in channelopathy eg Brugada syndrome, LQT syndrome), normal echocardiogram and normal coronary angiogram. This comprises 10% of all patients referred for evaluation of VT. They commonly originate from myocardial regions around RV and LV outflow tract near aortic and pulmonary cusp but sometimes from epicardial aspect from LV summit. LV summit is the triangular region of LV epicardium with the apex at the bifurcation between the Left anterior descending (LAD) and Left Circumflex coronary (LCx) arteries, and the base formed by an arc connecting the first septal perforator branch of the LAD with the LCx, triangle bisected by great cardiac vein. At one end of the spectrum this may present with frequent isolated PVCs, couplets or salvos of non-sustained VT present predominantly at rest or following a period of exercise, decreases at peak exercise whereas other end of the spectrum it manifests as paroxysm of sustained VT precipitated by exercise or emotional stress with infrequent PVCs and predominantly normal sinus rhythm during resting phase [2].
Among 3 well described mechanism of arrhythmia (Automaticity, ReEntry, Triggered activity), it is postulated outflow tract VT mechanism is catecholamine induced cyclic adenosine monophosphate (cAMP) mediated delayed after depolarization triggered activity. It is often of focal origin distinguishing it from the reentrant form of VT (e.g. scar related reentrant VT, fascicular VT, Bundle branch reentrant VT etc).
Usually affected patients are relatively young manifesting between 3rd to 5th decades of life with more prevalence among men than women. Prognosis is excellent with rare risk of sudden cardiac death; spontaneous remission may be seen in 5%-20%. PVC induced cardiomyopathy may be seen if high PVC burden (>15-20%). LV dysfunction is usually reversible after appropriate PVC/VT suppression.
12 Lead ECG (Figure 1), has a classical characteristic pattern (LBBB, Inferior axis i.e. tall R waves in Lead II, III, aVF, and QS complex in aVR and aVL). There are several well described ECG characteristics that help to distinguish between RVOT versus LVOT exit, or identify PVCs originating from commissural region of RCC and LCC. Echocardiogram and coronary angiogram are typically normal. Cardiac MRI is rarely necessary for diagnosis but may be helpful to rule out arrhythmogenic right ventricular cardiomyopathy, Epicardial RVOT dysplasia that may be seen with Brugada syndrome, sarcoidosis, amyloidosis etc.

Figure 1: Example of outflow tract PVC
Catheter ablation of outflow tract VT is effective, successful with low complication rate, low risk of recurrence. In a multicenter trial, catheter ablation showed acute success in 84% and arrhythmia suppression in 85% in mean follow up duration of 1.9 years [3]. Ablation is preferred particularly in highly symptomatic patients, PVC induced cardiomyopathy, or when medical management with beta blocker/calcium channel blocker, or antiarrhythmic medications is ineffective, or not tolerated or not desired. Due to the focal nature of the arrhythmia, PVC exit site is localized with local activation time mapping of the outflow tract. For this reason, it is necessary that patient has spontaneous or inducible PVCs with medications like Isoproterenol during the ablation procedure to allow accurate mapping. Several 3-dimensional electroanatomic sophisticated mapping systems are available (CARTO; Biocense Webster, RHYTHMIA; Boston Scientific, EnSite; Abott) with each having their unique algorithm. Utilization of intracardiac echocardiogram further allows adequate visualization and catheter navigation, confirming adequate tissue contact, minimize fluoroscopy and enhance safety with reduced complications such as pericardial effusion. Often these procedures are performed under conscious sedation as deeper sedation or general anesthesia results in PVC suppression making it difficult to map. Pace mapping can be alternative but is less accurate due to inherent fallacies. Radiofrequency ablation with 4 mm Tip open irrigated catheter for 45-60 seconds is necessary to effectively suppress PVCs. While ablating from Aortic cusp, care should be taken to avoid inadvertent ablation near coronary ostium. In symptomatic patients with frequent PVCs from RVOT, catheter ablation showed higher efficacy compared to pharmacotherapy with metoprolol or propafenone [4-14,1]. Due to high ablation success rate with low complication rate, current guideline recommended catheter ablation for symptomatic frequent PVC as preferred therapy in suitable symptomatic patient [1]. Complication rates are low with most common complication being vascular access site complications such as groin hematoma, bleeding, pseudoaneurysm, AV fistula etc which is seen much less at modern time due to wider adoption of ultrasound guided vascular access in most practices, availability of various vascular closure devices etc. Other complications are pericardial effusion which sometimes may require percutaneous catheter drainage or surgical intervention, cerebral embolic stroke, need for pacemaker due to iatrogenic Atrioventricular block if ablating close to penetrating bundle of his, death etc. Hayashi et al. [15-28], reported in a retrospective observational analysis that there has been increase in patients undergoing catheter ablation for outflow tract PVC or VT with more ablations performed at non–right ventricular outflow tract locations, over time, single procedure success has improved and complications have remained limited.
Papillary Muscle PVC and Fascicular VT
Fascicular VT also known as verapamil sensitive VT is a form of Idiopathic reentrant VT that occurs in younger patients (15-40 years, unusual after 55 years), relatively benign clinical course, and has an excellent prognosis. Tachycardia circuit commonly involves the region of left posterior fascicle (90%), less commonly Left anterior fascicle, rarely arises from fascicular locations high in the septum. Clinical symptoms include palpitation, lightheadedness, fatigue, dyspnea, rarely syncope or cardiac arrest. VT is catecholamine sensitive and hence occurs during physical or emotional stress, though it may occur during rest. Symptoms are usually paroxysmal lasting for minutes to hours, seldom incessant. Because Fascicular VT utilizes the fascicular purkinje conduction system, ECG is characterized by a relatively narrow QRS duration with a short intrinsicoid deflection (RS interval). Left posterior fascicular VT exhibits RBBB-Left anterior fascicular block pattern and superior axis, whereas Left anterior fascicular VT exhibits RBBB configuration with right axis deviation. Several features can be helpful in distinguishing Left posterior fascicular VT from SVT with aberrant conduction when classic hallmark features of VT such as AV dissociation is absent. An atypical RBBB pattern (no rsR′, or R larger than R′), the presence of QS patterns in lead V 6, positive QRS in lead aVR are some of the signs helpful in differentiating LPF-VT from SVT with RBBB and LAF aberration (Figure 2).
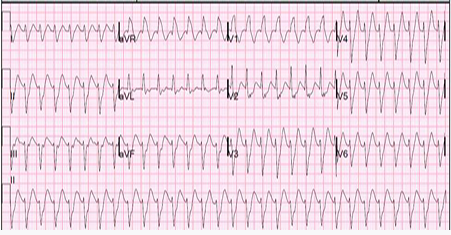
Figure 2: Left Posterior Fascicular VT: ECG shows RBBB, Left axis deviation and superior axis (positive aVR, negative in inferior leads). QRS complex are relatively narrow and short intrinsicoid deflection compared to VT seen in structural normal heart due to early engage ment of His purkinje conduction system, and hence usually VT is fast approximately 150-200 bpm.
Catheter ablation acute success rate in case of fascicular VT is 90%. Nogami et al reported success and recurrence rates are 97% and 4%, respectively, for LPF VT; 90% and 11%, respectively, for LAF VT; and 100% and 2.5%, respectively, for left upper septal fascicular VT [12,13]. Usually, a transaortic approach is used to advance ablation catheter into Left Ventricle. Radiofrequency ablation using an open irrigated catheter is commonly used. Different mapping strategies eg activation mapping, substrate mapping, entrainment mapping is effective in identifying target for ablation. Distal most fascicular potentials of left posterior fascicle are preferred target for ablation associate with high success rate.
Papillary muscle VT is idiopathic focal (non reentrant) mechanism that commonly manifest as frequent PVCs. ECG morphology shows similar RBBB pattern to fascicular VT but much wider, and there is often mid precordial transition seen. This is also catecholamine sensitive and often exercise induced. Because papillary muscle is a thick fleshy structure achieving adequate energy penetration to deeper intramural foci with Radio frequency ablation can be challenging sometime. Papillary muscle contraction makes catheter stability difficult. Intracardiac echocardiogram is helpful to visualize adequacy of catheter contact. Acute procedural success rate varies between 60%-90% with recurrence rate of 50%-70%.
Mitral/Tricuspid Annular PVC/VT
PVC/VT originating from Mitral and Tricuspid valve annular region represent around 5%-8% of idiopathic ventricular arrhythmia. Mechanism is predominantly triggered activity or automaticity. ECG in Mitral annular PVC shows RBBB with predominantly positive QRS complex V1-V6. Majority of Mitral annular VT is anterolateral and hence predominantly negative QRS complex in lateral leads (L1, aVL) is seen, a positive polarity in L1 and aVL may be seen in septal origin. Axis is inferior (positive in II,III,aVF) in anterior mitral annular PVC whereas negative polarity in inferior lead may be seen in posterior or postern-septal mitral annular PVC/VT. One classic sign is notching at late phase of QRS complex (Figure 3), seen in PVCs originating from LV free wall aspect. Tricuspid annular PVCs demonstrate LBBB morphology (suggesting RV origin), strongly positive in lateral leads like L1 as the wavefront is propagating from right to left parallel to L1. Catheter ablation is often successful but recurrence rate up to 8% [30], was seen in one series. Tricuspid annular VT from RV free wall has a greater success rate compared to septal origin [12], due to proximity to AV node and his purkinje system increasing risk of iatrogenic complete heart block during ablation.
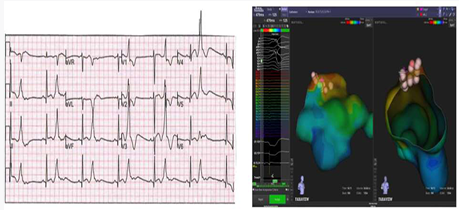
Figure 3: Mitral annular PVC. 12 Lead ECG shows RBBB pattern (suggest LV exit) with inferior axis (+ve in II, III, aVF and -ve in aVR and aVL) suggesting anterior exit, monophonic R wave in V1 with predominant positive R wave in all precordial leads (V1-6) suggesting basal LV exit (mitral annular or subvalvular region), Predominantly negative polarity in lateral leads (L1, aVL) suggest lateral exit. Notching at the late phase of the QRS complex in inferior leads is seen in PVC originating from the free wall portion of LV [29]. Side panel shows the 3 D electroanatomic activation nap of this PVC in Right anterior oblique projection and Poster-anterior projection. As predicted from ECG, PVC was localized to anterior mitral annulus (RAO projection) and lateral free wall LV (PA projection looking into mitral valve and LV from LA). Ablation lesion are shown by the red pale pink circles. Earliest local ventricular electrogram preceding the PVC were found here and ablation here resulted in successful ablation.
Bundle Branch reentrant VT (BBRVT)
Bundle Branch Reentrant VT is a macro reentrant monomorphic VT often very fast (200-300 bpm) associated with hemodynamic collapse, syncope, and/or cardiac arrest that is seen more often in patients with dilated cardiomyopathy but can be seen in other conditions such as valvular heart disease, MI, myotonic dystrophy, Brugada syndrome, and ARVC among others. Tachycardia circuit involves His bundle, Right and left Bundle and ventricular septal myocardium. Infrahisian conduction delay and a dilated heart from cardiomyopathy are two predisposing substrate for BBRVT to occur as dilated heart causes an anatomically longer pathway, and infrahisian conduction disease creates differential conduction velocity and refractoriness between two limbs of the tachycardia circuit (Right and left bundle brances). It can be counterclockwise (common) using Right bundle as antegrade limb, then propagating through septal myocardium and engaging the Left bundle as retrograde limb and turing around at the bundle of his or clockwise (less common).
Usually BBRVT is very fast (200-300 beats per minute) as it utilizes the HPS-Purkinje conduction system. Since this is seen more commonly in patients with poor ventricular function, it is poorly tolerated hemodynamically, hence majority of patients experience syncope or cardiac arrest on presentation.
Almost all patients with BBRVT demonstrate some baseline intraventricular conduction abnormality, more common being prolong PR and LBBB during sinus rhythm. ECG during VT has a LBBB pattern similar to during sinus rhythm (common pattern during counterclockwise BBRVT), rapid intrinsicoid deflection, normal or left axis deviation. RBBB morphology BBRVT (less common, clockwise) may have normal or rightward axis.
AAD is less effective in BBRVT. Catheter ablation is very successful in eliminating BBRVT and regarded first line therapy [1,2]. However, because 45% of BBR VT patients also has poor LV systolic function predisposing them to other myocardial VT, ICD implantation for secondary prevention is strongly recommended. Usual target for ablation is either RB or LB. RB is an easier and preferred choice. Though there may be concern for AV block after ablation of RB because of baseline conduction abnormality in the LB, LB can still maintain 1:1 AV conduction during NSR following ablation of the RB. RB is superficial, slender and long and mapping the RB electrogram potential delineate the target for ablation. LB is broad, thicker and shows a wide arborized pattern and hence broad area of ablation is required. Radiofrequency catheter ablation using 4 mm tip irrigated catheter is commonly used.
The acute success rate of BBR VT ablation approaches 100%. Non Inducibility of BBR, development of an RBBB pattern are usual endpoint of ablation. Reversal of his bundle activation during pacing from RV apex is seen after successful ablation of RB. Usually, the quadripolar catheter at his bundle get activated in distal to proximal direction during RV pacing. After successful ablation of RB, during RV pacing depolarization wavefront has to cross the interventricular septum, propagate up the LV, turn around at His Bundle and activate the His Bundle in an antegrade manner (proximal to distal).
Epicardial VT ablation
Unlike Post MI VT where wedge shaped necrotic wavefront progresses from subendocardium to epicardium, in patients with dilated cardiomyopathy, chagas disease, arrhythmogenic right ventricular cardiomyopathy, healed myocarditis etc. VT substrate is often mid myocardium to epicardial. So, need for epicardial mapping and ablation is not infrequent after failed endocardial ablation. In dilated cardiomyopathy larger epicardial scars mostly around mitral valve annulus is seen. In ARVC there is fibrofatty replacement with subepicardium to midmural involvement around tricuspid valve apparatus and RVOT region. Various ECG characteristics may give clue to an epicardial substrate which rely on the concept that ventricular wavefront that begins at the epicardium propagate very slowly till it can engage an efficiently conducting purkinje fiber system resulting in wide bizarre slurred QRS complex often manifested by delta wave, or long R wave peak time, presence of Q wave in Lead I, absence of Q waves in any inferior leads in VT with basal superior exit, or presence of Q waves in inferior leads in basal inferior VT etc. Cardiac imaging such as MRI, cardiac CT, nuclear scintigraphy etc may help to identify epicardial substrate. Usually percutaneous subxiphoid approach provide access to the pericardial space, except in patients with previous cardiac surgery where there may be pericardial fibrosis and adhesions. Several preprocedural clinical factors predict need for epicardial approach e.g. presence of intracavitary thrombus, presence of mechanical aortic and mitral valve, prior failed endocardial ablation. Energy modality used for epicardial VT ablation is mostly RF though Cryo ablation is investigational because of the advantage that there absence of cooling blood flow in the pericardial space enhances the formation of the cryolesion, and Cryo is less prone to cause coronary artery injury. However human experience is limited. On the other hand surgical cryoablation with hand held probes are common. With RF ablation, irrigation fluid from ablation catheter should be periodically drained to avoid cardiac tamponade. Complications of epicardial ablation is mostly hemopericardium, RV wall perforation, coronary artery injury, pericarditis, phrenic nerve injury, pneumopericardium, intra-abdominal visceral injury etc. Pneumopericardium rarely cause tamponade however it significantly may increase transthoracic defibrillation threshold which may have serious deleterious effect because of frequent need for cardioversion during VT induction and activation/entrainment mapping.
Stereotactic body radiation therapy (SBRT)
Several clinical trials have shown Catheter ablation being effective in reducing VT burden, reduce incidence of appropriate ICD shock and improving quality of life. However, catheter ablation may not be effective in certain patients specially in deep intramural or subepicardial substrate, proximity to coronary arteries etc. SBRT could be an option after failed catheter ablation. Cuculich et al., published data on five patients with refractory ventricular tachycardia, noninvasive treatment with electrophysiologyguided cardiac radioablation markedly reduced the burden of ventricular tachycardia [7]. Neuwirth et al., reported on a larger patient sample (10 patients) with 28 month follow up on safety and efficacy of SBRT. This case series showed longterm safety and effectiveness for VT ablation in structural heart disease inaccessible to catheter ablation [8]. Robinson [10] et al., conducted prospective trial on 19 patients which showed Noninvasive electrophysiology-guided cardiac radioablation is associated with markedly reduced ventricular arrhythmia burden with modest short-term risks, reduction in antiarrhythmic drug use, and improvement in quality of life. A systematic review including 13 clinical trials [9], showed Stereotactic radioablation for VT may be safe and effective with short term success in reduction of sustained VT/VF among patients with therapy refractory VT. Arrhythmogenic target for ablation is usually based on exporting previous electroanatomic mapping during catheter ablation combined with anatomical scar imaging (echocardiography, computed tomography (CT), magnetic resonance imaging (MRI), and/or positron emission tomography (PET)/scintigraphy imaging). Respiratory and cardiac motion of the target area adds challenge to targeted treatment delivery. Currently there is limited data on radiation effect on normal and diseased heart, possible acute and late radiation-related effects of STAR, lower dose (20-25 Gy) may affect conduction versus higher dose (30Gy) may induce scar formation. These different mechanisms further complicate accurate recommendations for the prescription dose, desired dose (in)homogeneity, and the maximum dose. To provide a pooled treatment database to evaluate patterns of practice and outcomes of STAR and finally to harmonize STAR, STOPSTORM [11], consortium has been established in Europe comprising of 31 clinical and research institutions. As more data emerge, SBRT holds a promising future for therapy refractory VT.
Surgical Ablation
Despite Radiofrequency catheter ablation with conventional Endocardial and/or Epicardial approach, VT may be recurrent. In patients with prior cardiac surgery or pericarditis, percutaneous pericardial access may not be possible. In patients with ineffective or failed catheter ablation, surgical approach may be helpful particularly if patient is undergoing concomitant cardiac surgery for some other alternative indication. Surgical cryoablation [1,21,22], with lateral thoracotomy (preferred in lateral or posterior substrate) or sternotomy, along with localization of substrate with VT induction when patient is off cardiopulmonary bypass with portable electroanatomic mapping system in operating room can be performed. In patients with pericardial adhesion, creation of a subxiphoid window can provide access to epicardial space, particularly apical and inferior substrate is easy to reach with this approach and can be performed in the electrophysiology laboratory. Anter [20] et al., reported a series of 8 patients who had recurrent sustained VT despite antiarrhythmic drugs and endocardial and/or epicardial ablation procedures. Surgical cryoablation was applied to previously identified substrate with electroanatomic mapping during previous ablation procedure. There were no significant perioperative complications. During a mean follow-up period of 23±6 months (range, 15 to 34 months), 6 patients had significant reduction in VT burden as evident by a reduced number of implantable cardioverter-defibrillator shocks after ablation (6.6 to 0.6 shocks per patient; P=0.026). Two patients died, one of progressive heart failure and one of sepsis. In a large sample of 444 patients of VT with prior MI, William Stevenson [22], reported safety-efficacy, role of epicardial ablation and role of surgical ablation with outcome data in a mean follow up over 26 months.
Cardiac sympathetic denervation
Autonomic nervous system influences heart rate, and autonomic nervous system imbalance plays a role in onset or maintenance of ventricular arrhythmia with its sympathetic arm mediated by cervicothoracic paravertebral sympathetic ganglion, and parasympathetic arm mediated by vagus nerve in variety of VAs including in structurally normal heart e.g. idiopathic catecholaminergic outflow tract VT which are very much responsive to beta blocker therapy, channelopathies e.g. Brugada syndrome or idiopathic VF Isoproterenol during VT strom can abolish recurrent arrhythmia, or in patients with structural heart disease. Transient Cervical sympathetic denervation can be achieved epidural bupivacaine in T1-2, T2-3 epidural space. Ackerman et al. [22], in a retrospective chart review of 52 patients with long QT syndrome showed Left cardiac sympathetic denervation showed significant reduction in VA burden but also identified a high-risk group of LQTS patients 50% of whom experienced breakthrough events post LCSD and so opined LCSD must not be viewed as curative or as an alternative in implantable cardioverter defibrillator for high-risk patients. Percutaneous stellate ganglion block is successful in electrical storm in post MI patient and can be used as a bridge till definitive therapy. Persistent Cardiac sympathetic denervation can be achieved by video assisted thoracoscopic resection of lower third of stellate ganglion, T2 to T4/5 level or nerve of kuntz [1]. In a retrospective analysis study on 121 patients with SHD in 5 international centers, Shivkumar et al. [23], reported left or bilateral surgical CSD decreased sustained VT and ICD shock recurrence in patients with refractory VT.
Salvage DC Ablation
In a limited case series of 4 patients who failed multiple Radiofrequency ablation for VT previously, author [24], reported a single center experience of salvage DC ablation with biphasic energy. During a follow up of 3 months to 1 year no recurrent VT was observed. In this limited series it was observed DC ablation may be safely used in refractory VT however large trials with proper randomization studies are necessary prior to performing such procedures routinely. With more number of DC pulse application there is a risk of transient hypotension, worsening heart failure and death.
Pulsed Field Ablation
Pulsed Field ablation is non thermal modality of ablation causing irreversible electroporation. This technology is now FDA approved and well established backed up by robust clinical evidence and accepted as almost standard of care for atrial fibrillation ablation due to cardiac tissue selectivity thus avoiding collateral damage e.g. esophageal or phrenic nerve injury, better efficacy etc. Safety and feasibility of PFA technology for VA is still experimental and hence RF ablation still remains the standard of care for VA ablation. However, RF ablation has its inherent limitation due to point-by-point ablation with smaller area of focal ablation potentially leaving gaps between ablation lesions, catheter stability, inadequate depth in case of deeper myocardial substrate etc. It is intuitive that PFA with a pentaspline catheter will cover a broader substrate area of endocardial substrate with single shot application and may even create deeper lesion depth but coronary spasm remains a serious concern. Studies on animal models showed similar lesion depth with both PFA and RFA but PFA had better penetration in scar tissue and Fat. A case report of histologic lesion analysis after in human application of both PFA and RFA showed similar findings with animal model. This showed similar lesion depth but different lesion characteristic with apoptotic-like cellular lesions and notable lack of inflammation in PFA [28]. Non gated PFA application had potential to induce VF which could be avoided with QRS gating. Santangeli [27] et al., reported first and largest US series including 11 patients with pentaspline PFA system (FARAWAVE, Boston Scientific). Study included 11 male patients, mean EF 35%, 9 patients had scar related VT, 7 had ischemic cardiomyopathy, 2 non ischemic cardiomyopathy, 1 patient had ARVC, 2 patients had papillary muscle PVC (1 from anterolateral papillary muscle, 1 from postero-medial papillary muscle). Acute procedural success (non inducibility of VT) was seen in all patients with no procedural complications especially coronary spasm, new valvular dysfunction, conduction disturbance, vascular complication, or worsening of renal function seen. In a mean follow up of 205+/-55 days there were no death, two patients had recurrent VT and 1 had recurrent Postero medial papillary muscle PVC. Limited by extremely small sample size and lack of long term follow up data, this first US case series however signaled towards a favorable outcome and feasibility of PFA as a future technique of VT ablation. FARAWAVE PFA catheter is non steerable and reaching basal and posterior LV segments were difficult where touch up RF ablation was necessary. Newer catheter design with focal delivery of pulsed field energy, steerable catheter are under investigation and when available may hold promise for this novel technology in VA ablation. Larger sample size, long term follows up data will be necessary before adopting PFA for VA ablation.
Operator and Institutional experience requirement
ACC/AHA/HRS guideline have laid down the institutional requirement and competency standards for institutions to be able to perform VA ablation procedures. Electrophysiology training in an advanced program performing high volume VT ablation is necessary for physician. Presence of multidisciplinary support including interventional cardiology, advanced heart failure, cardiomyopathy and transplant program, cardiac surgery program with ability for mechanical circulatory support, emergent sternotomy if necessary, cardiac anesthesiologist, cardiac critical care for post procedural management, cardiac imaging with ability for performing Cardiac CT/MRI, PET/CT etc are all of paramount importance. As conceivable, henceforth VT ablation is an exceptionally complex procedure that needs tertiary highly specialized center with high operational expertise with electrophysiology laboratory staff and personnel who are experienced and familiar with complexity of such procedures. VT network is a concept of network of tertiary regional centers with capability of performing all techniques of VT and electrical storm ablation to facilitate logistics for optimizing patient flow and referral.
Cost Benefit Analysis
While catheter ablation of VT may be associated with high upfront cost, when compared to prolong amiodarone use on a long term management basis cost benefit ratio is favorable to catheter ablation because of increased quality of life post ablation, reduced need for prolonged AAD and monitoring and associated health care burden related to side effects. Calkins et al., reported catheter ablation appears to be a cost-effective alternative to amiodarone for treating VT patients from a societal perspective yielding a cost-effectiveness ratio of $20 923 per Quality Adjusted Life Year [25], gained for ablation compared with amiodarone. Consistent finding was seen in another study by Stevenson [26], et al., where cost effectiveness of catheter ablation was compared to escalation of antiarrhythmic drug in patient population from VANISH randomized controlled trial. Catheter ablation was seen to be cost effective compared with escalation of AAD for total trial population, result particularly manifest in the subgroup who had recurrence of arrhythmia despite being on amiodarone.
CONCLUSION
With increasing life expectancy, burden of Coronary artery disease, Congestive heart failure VT has emerged as a major cause of sudden cardiac death. Though AADs are effective to limited extent and ICD implantation is highly effective in prevention of sudden cardiac death, recurrent ICD shock or escalation of AAD is often necessary with progressive VT burden. Recurrent ATP therapy or ICD shock is associated with increased mortality, poor quality of life, psychologically distressful symptoms. Catheter ablation is being increasingly utilized and effective in minimizing ICD shock, or improve quality of life. Future direction hold promise for novel ablation techniques such as Pulsed Field Ablation, which is currently being investigated for ventricular arrhythmia ablation. Appropriate diagnosis of VT etiology and mechanism is essential in optimizing 3 Dimensional electroanatomic mapping and a successful ablation therapy.
How to Cite
References
URL: https://www.jacc.org/doi/10.1016/j.jacc.2017.10.054
URL: https://www.sciencedirect.com/book/monograph/9780323523561/clinical-arrhythmology-and-electrophysiology
URL: https://pubmed.ncbi.nlm.nih.gov/29759353/
URL: https://pubmed.ncbi.nlm.nih.gov/31082362/
URL: https://pubmed.ncbi.nlm.nih.gov/27149033/
URL: https://pubmed.ncbi.nlm.nih.gov/39555820/
URL: https://pubmed.ncbi.nlm.nih.gov/29236642/
URL: https://pubmed.ncbi.nlm.nih.gov/31121018/
URL: https://pubmed.ncbi.nlm.nih.gov/34233215/
URL: https://pubmed.ncbi.nlm.nih.gov/30586734/
URL: https://pubmed.ncbi.nlm.nih.gov/36879464/
URL: https://www.sciencedirect.com/book/monograph/9780323529921/catheter-ablation-of-cardiac-arrhythmias
URL: https://pubmed.ncbi.nlm.nih.gov/28292752/
URL: https://pubmed.ncbi.nlm.nih.gov/24523413/
URL: https://pubmed.ncbi.nlm.nih.gov/32081227/
URL: https://pubmed.ncbi.nlm.nih.gov/10841242/
URL: https://pubmed.ncbi.nlm.nih.gov/19064682/
URL: https://pubmed.ncbi.nlm.nih.gov/24958396/
URL: https://pubmed.ncbi.nlm.nih.gov/38102318/
URL: https://pubmed.ncbi.nlm.nih.gov/21673018/
URL: https://pubmed.ncbi.nlm.nih.gov/24107459/
URL: https://pubmed.ncbi.nlm.nih.gov/23728945/
URL: https://pubmed.ncbi.nlm.nih.gov/28641796/
URL: https://academic.oup.com/eurheartj/article/41/Supplement_2/ehaa946.0410/6002524
URL: https://pubmed.ncbi.nlm.nih.gov/10645924/
URL: https://pubmed.ncbi.nlm.nih.gov/29798795/
URL: https://pubmed.ncbi.nlm.nih.gov/40516776/
URL: https://pubmed.ncbi.nlm.nih.gov/37488032/
URL: https://pubmed.ncbi.nlm.nih.gov/15766824/
URL: https://pubmed.ncbi.nlm.nih.gov/16191111/