Abstract
Background
Both mitral regurgitation (MR) and tricuspid regurgitation (TR) frequently exist in patients with Atrial Fibrillation (AF). But whether valvular regurgitation causes AF or vice versa is unclear.
Atrial fibrillation is the most common rhythm disturbance diagnosed in clinical practice. As the population ages Atrial Fibrillation (AF) is predicted to affect 6-12 million people in the United States by 20501. The main focus on the clinical complications of AF has included: stroke, Heart Failure (HF) and sudden Cardiac Death (SCD). The occurrence of Valvular regurgitation in patients with AF has been less studied.
There are a few studies which have evaluated improvement of functional mitral valve regurgitation with a rhythm control strategy2, 3, there is some evidence that tricuspid regurgitation may be associated with AF4, but to the best of our knowledge there has been no study performed to evaluate response of tricuspid regurgitation to a rhythm control strategy.
Primary MR/TR is when the leaflets or the sub valvular apparatus are structurally abnormal causing leaf let malcoaptation. Functional valvular regurgitation occurs when the leaflets or the sub valvular apparatus are structurally normal and leaf let malcoaptation is related to global or regional ventricular remodeling that displaces the papillary muscles, tethers the leaflets, or by reduction in ventricular closing forces. We were interested in whether restoration of Sinus Rhythm (SR) could result in reverse remodeling in the patients with AF and functional valvular regurgitation.
Objective
To evaluate the effect of a rhythm control strategy involving AF ablation on mitral or tricuspid regurgitation which is at least moderate in severity?
Methods
Patients with moderate or severe, mitral or tricuspid regurgitation and atrial fibrillation at our center underwent a rhythm control strategy with an ablation procedure. Anti-arrhythmic drugs were used at the discretion of the treating physician. The severities of mitral or tricuspid regurgitation were assessed using the 2017 American Society of Echocardiography guidelines.
Results
30 patients with moderate or severe mitral regurgitation underwent a rhythm control strategy with ablation procedure. 90% of patients (27/30) showed an improvement in the severity of regurgitation with 6 patients demonstrating a decrease in mitral regurgitation from severe to mild and 21 patients from moderate to mild. There were 19 patients with moderate or severe tricuspid regurgitation. 15/19 (79%) patients improved. 4 patients improved their tricuspid regurgitation from severe to mild. 11 patients improved their TR from moderate to mild. None of the patients showed a worsening of either mitral or tricuspid regurgitation from baseline. All patients who had improvement in their valvular regurgitation also showed an improvement in their functional capacity.
Conclusion
Restoration of sinus rhythm significantly improved valvular regurgitation and functional capacity in a majority of patients without any valvular interventions suggesting a pathophysiologic role of atrial fibrillation in development of valvular regurgitation.
Keywords
Five Clinical Cases
Case 1: MM
Clinical presentation: 67-year-old male presents with heart failure (HF) manifest as severe shortness of breath at rest.
Blood pressure 100/70 and irregularly irregular rhythm with heart rate = 97 bpm. Elevated JVP. 3/6 mitral regurgitation murmur, Bibasilar rales, and no peripheral edema. (Figure 1)
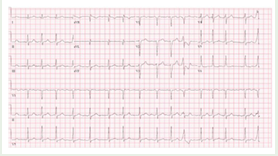
Figure 1: ECG: Atrial fibrillation
Echocardiogram: Increased LV cavity size, mitral annular dilation, and severe functional mitral regurgitation. LVEF = 25 (Figure 2)
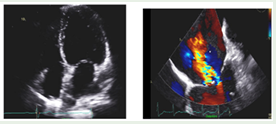
Figure 2: TTE with apical 4-chamber view demonstrating MV annular dilation and esophageal TEE view with severe mitral regurgitation
Cine 1: Atrial fibrillation (AF) with ventricular response (VR) between 105-112 bpm
Trans Esophageal Echocardiogram (TEE) esophageal view demonstrating Mitral Valve (MV) annulus dilation
With severe, central (functional) Mitral Regurgitation (MR) with color flow
a) Cardio version: Successful cardio version from atrial fibrillation to sinus rhythm (Figure 3).

Figure 3: ECG: Sinus Rhythm
b) Repeat Echocardiogram: Mild increase in LV size and with LVEF = 40%. Mild mitral regurgitation (Figure 4).
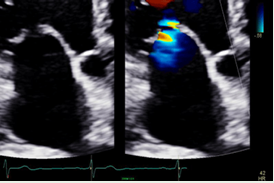
Figure 4: In SR with decreased MV annulus dimension and mild MR
Table 1: Reversal of Severe MR with Significant Cardiac
|
Echocardiogram in AF (Mean for 6 patients) |
Echocardiogram after restoration of sinus rhythm (Mean for 6 patients) |
Months (Mean duration) |
|
|
Severity of mitral regurgitation |
Severe |
Trace to mild |
8 Months |
|
Mitral valve annular diameter |
47.3 mm |
32 mm |
|
|
Left ventricular ejection fraction |
19% |
58% |
|
|
Left atrial volume index |
51mL/m2 (Severely enlarged) |
38 mL/m2 (Mildly enlarged) |
|
|
Left ventricular size |
67.5 mm |
56.8 mm |
|
|
Right ventricular size |
Normal to mildly enlarged |
Normal size |
|
|
RV systolic function (Pulsed Doppler S wave) |
9.3 cm/second |
19.3 cm/second |
|
|
Right atrial size |
Moderately enlarged |
Normal to mildly enlarged |
|
|
Inferior vena cava |
Plethoric |
Normal |
|
|
NYHA functional class |
Class IV |
Class I- II |
Cine 2: Sinus rhythm (SR) with VR approximately 42 bpm. Transthoracic echocardiogram (TTE) demonstrating mild (central) MR with color flow
a) Coronary status: Normal nuclear perfusions scan
b) Ablation: Pulmonary Vein Isolation, Cavo Tricuspid isthmus ablation.
c) Clinical follows up: Class 1 functional status
Case 2:
PA Clinical presentation: 77 -year-old male presents with heart failure (HF) manifest as exertional shortness of breath with rapid heart rate.
Blood pressure 120/80 and irregularly irregular rhythm with heart rate = 110 bpm. Elevated JVP, 2/6 murmur right sternal border 4th ICS, Elevated JVP, ascites, and (2+) peripheral edema (Figure5).
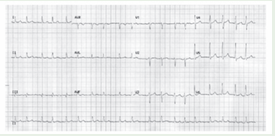
Figure 5: ECG: Atrial Fibrillation
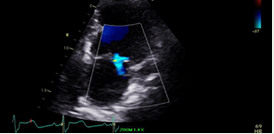
Echocardiogram: Remodeled RV cavity with RV enlargement.Depressed RV function.TV annulus dilation with severe tricuspid regurgitation (Figure6).
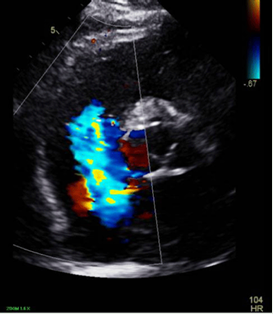
Figure 6: Parasternal short-axis view at the AV level revealing severe TR
Table 2: : Reversal of Severe TR with Significant Cardiac RemodelingRemodeling
|
Echocardiogram in AF (Mean for 4 patients) |
Echocardiogram after restoration of sinus rhythm (Mean for 4 patients) |
Months (Mean duration) |
|
|
Severity of tricuspid regurgitation |
Severe |
Mild |
26.5 months |
|
Tricuspid valve annular diameter |
47.5 mm |
37.5 mm |
|
|
Right atrial size |
Severe enlargement |
Mild enlargement |
|
|
Right ventricular size |
Moderate enlargement |
Normal size |
|
|
Right ventricular systolic function (Pulsed Doppler S wave) |
7.25 cm/second |
19.25 cm/second |
|
|
Left ventricular ejection fraction |
31% |
58% |
|
|
Left atrial volume index |
41.25 mL/m2 |
35.25 mL/m2 |
|
|
Inferior vena cava |
Plethoric |
Normal |
|
|
NYHA Functional Class |
Class III- IV |
Class I-II |
Cine 3: AF with VR approximately 100-105 bpm. TTE short-axis view at the level of the aortic valve demonstrating severe tricuspid regurgitation (TR) with color flow
a) Cardio version: to Sinus rhythm
b) Ablation: Pulmonary Vein Isolation and Cavotricuspid isthmus ablation (Figure7).
Figure 7: ECG
c) Repeat Echocardiogram: Normal RV size and function with trivial TR (Figure8).
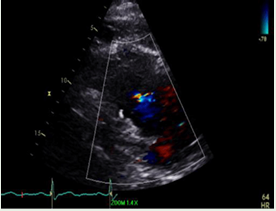
Figure 8: RV inflow view revealing trace TR
Cine 4: SR with VR = 66 bpm
TTE apical 4-chamber view demonstrating trace TR with color flow
a) Coronary status: Normal coronary arteries with angiography
b) Ablation: Successful
c) Clinical follows up: Class 1 functional status
Case 3:
SB Clinical presentation:
52 -year-old female presents with heart failure (HF) manifest as class 3 shortness of breath with rapid heart rate. Blood pressure 90/60 and irregularly irregular rhythm with heart rate = 150- 180 bpm. Elevated JVP, 3/6 mitral regurgitation, No peripheral edema (Figure 9).
Figure 9: ECG: Atrial fibrillation
Echocardiogram: Increased LV cavity size, mitral annular dilation with severe functional mitral regurgitation. LVEF = 35% (Figure 10).
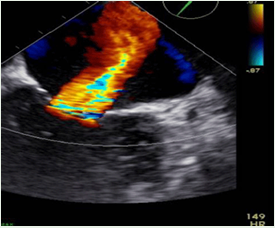
Figure 10: TEE reveling severe mitral regurgitation
Cine5: AF with VR approximately 130 bpm
TTE apical 4-chamber view revealing annular dilation with severe central MR
a) Cardio version to Sinus rhythm (Figure 11)
Figure 11: ECG: Sinus Rhythm
b) Repeat Echocardiogram: Normal LV size and function with trivial MR; LVEF = 60% (Figure 12)
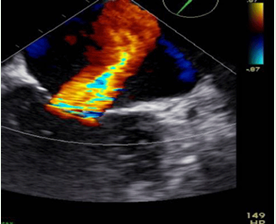
Figure 12: TTE revealing mild mitral regurgitation
Cine 6: SR with VR = 60 bpm
TTE apical 4 chamber view demonstrating trace MR with color flow
a) Coronary status: Normal perfusion scans
b) Ablation: Pulmonary vein isolation
c) Clinical follows up: Class 1 functional status
Case 4: KN
Clinical presentation: 62 -year-old male presents with NYHA Class IV heart failure (HF) symptoms manifest as severe shortness of breath at rest with controlled heart rate. Patient was unable to lie flat.
Blood pressure 130/80 and irregularly irregular rhythm with heart rate = 97-100 bpm. Elevated JVP. 3/6 mitral regurgitation, No peripheral edema (Figure 13)
Figure 13: ECG: Atrial FibrillationECG: Atrial Fibrillation
Echocardiogram: Reveal severely increased LV cavity size, mitral annular dilation with severe functional mitral regurgitation. LVEF = 25% (Figure 14).
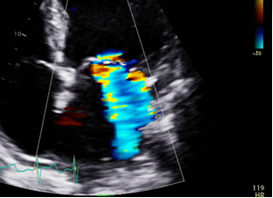
Figure 14: Severe Mitral Regurgitation
Cine 7: AF with VR = 112 bpm
TTE apical 4-chamber view demonstrating severe MR with color flow
a) Cardio version to Sinus rhythm
b) Ablation: Pulmonary vein isolation (Figure 15).
Figure 15: ECG: Sinus Rhythm
c) Repeat Echocardiogram: Normal LV size and function with mild MR; LVEF = 60% (Figure 16).
Cine 8: SR with VR = 69 bpm
TTE apical 4 chamber view with trace MR with color flow
a) Coronary status: Normal coronaries angiographically
b) Ablation: Successful
c) Clinical follow up: Class 1 functional status
Case 5: ES
Clinical presentation: 67 -year-old female presents with chest pain, heart failure (HF) manifest as class 3 shortness of breath with controlled heart rate. Patient was unable to lie flat.
Blood pressure 110/80 and irregularly irregular rhythm with heart rate = 70 -100 bpm. Elevated JVP. 3/6 mitral regurgitation, No peripheral edema (Figure 17).
Figure 17: ECG: Atrial Fibrillation
Echocardiogram: Increased LV cavity size, mild mitral annular dilation, and severe functional mitral regurgitation. LVEF = 45% (Figure 18).
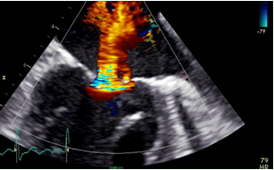
Figure 18: Severe Mitral Regurgitation
Cine 9: AF with VR = 90 bpm
TEE demonstrating annular dilation with severe (functional) MR with color flow
a) Cardio version to Sinus rhythm (Figure 19).
Figure 19: ECG: Sinus Rhythm
b) Repeat Echocardiogram: Normal LV size and function with mild MR; LVEF = 60% (Figure 20).
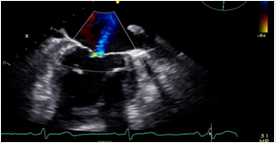
Figure 20: Mild Mitral Regurgitation
Cine 10: SR with VR = 50 bpm
TEE demonstrating trace to mild MR with color flow
a) Coronary status: Normal coronaries angiographically
b) Ablation: Pulmonary vein isolation, cavotricuspid isthmus ablation.
c) Clinical follows up: Class 1 functional status
Discussion
This case series generates a hypothesis that restoration of sinus rhythm in patients with atrial fibrillation and significant functional mitral regurgitation results in cardiac remodeling with decreased left ventricle chamber size, LAVI, mitral annular diameter, right atrial and ventricular size with dramatic improvement in left ventricular ejection fraction. Restoration of sinus rhythm was found to reverse severe Tricuspid regurgitation with a marked improvement in right sided chamber size, function and an improvement in left ventricular ejection fraction. The positive remodeling in sinus rhythm resulted in an improvement in patient functional capacity. These results should lead to further studies to reinforce the findings in this study.
How to Cite
References
URL: https://www.ncbi.nlm.nih.gov/pubmed/16818816
URL: https://www.ncbi.nlm.nih.gov/pubmed/23512117
URL: https://www.ncbi.nlm.nih.gov/pubmed/21939832
URL: https://www.ncbi.nlm.nih.gov/pubmed/22067002