Abstract
A 60-year-old female presented with dyspnea and chest pressure. Clinical presentation, laboratory data, and advanced cardiac imaging confirmed diagnosis of eosinophilic myocarditis, and obviate unnecessary invasive endomyocardial biopsy. She was treated with oral steroid and oral anticoagulation. Follow up cardiac MR showed resolution of the LV thrombus with improvement in endomyocardial inflammation.
Keywords
Case presentation
A 60-year-old female with past medical history of hypothyroidism, tobacco and methamphetamine use presented with a 3-day history of worsening dyspnea and chest pressure. After initial evaluation at outside hospital she was transferred to our facility for further evaluation and treatment. On arrival, her temperature was 98 F, her pulse was 104 beats/min, blood pressure was 100/60 mm Hg, and his arterial oxygen saturation was 94% on 2 L of nasal cannula oxygen. Physical examination revealed regular tachycardic heart rate with 3/6 systolic murmur over the apex; decrease bilateral basal lung sounds. She quit smoking one year ago, and her last drug use was two years ago. Differential diagnoses included acute coronary syndrome, Pulmonary embolism (PE), acute heart failure, acute myocarditis, pneumonia, endocarditis, and methamphetamine toxicity.
Electrocardiography showed sinus tachycardia with T wave inversion in V2 through V6. Initial lab showed elevated troponin 0.21 ng/ml and D dimer 0.73 mcg/ml. White blood cell count was elevated to 13,000 /µl with an elevated absolute eosinophil count of 1,900/µl (14.6%). Basal metabolic panel was normal. Urine drug screen was negative.
Computed tomography (CT), angiography of chest, at outside hospital, showed bilateral PE. Two-dimensional transthoracic echocardiography (TTE), and contrast TTE revealed left ventricle (LV), EF of 55%, grade 3 LV diastolic dysfunction, moderate mitral regurgitation, and LV regional wall motion abnormality with large laminated obliterating LV mid and apical thrombus (Figure 1a,1b,1c,1d) (Movie 1,2).
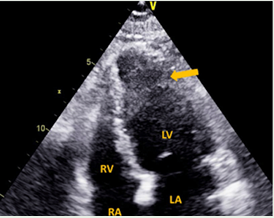
Figure 1a: Apical 4-chamber two-dimensional image at end-diastole showing thrombus obliterating apical LV cavity [arrowed]
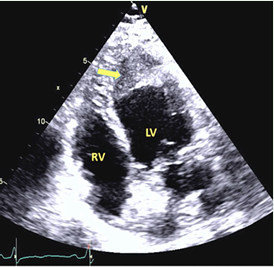
Figure 1b: Modified apical 4-chamber two-dimensional image at end-diastole showing thrombus obliterating apical LV cavity, extending into mid-anterolateral LV wall [arrowed]
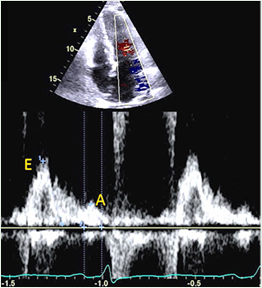
Figure 1c: Pulsed wave Doppler image of LV inflow velocity showing grade 3 LV diastolic dysfunction. Note E/A > 2, deceleration time 110 msec
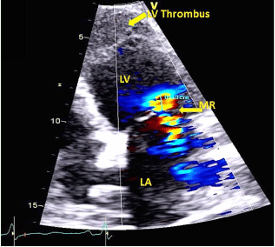
Figure 1d:Apical 4-chamber color Doppler image with baseline shift of Doppler scale showing moderate mitral regurgitation [PISA radius 0.89 cm, effective regurgitant orifice area 0.34 cm2]
Coronary angiogram was shoved normal coronary arteries. Cardiac magnetic resonance (CMR), showed LV endomyocardial edema on T2 weighted images, endomyocardial fibrosis, and extensive LV mural thrombus with obliteration of the LV cavity, features typical of eosinophilic myocarditis (EM) (Figure 2a,3a). Right ventricular function was preserved and the pericardium was normal on CMR.
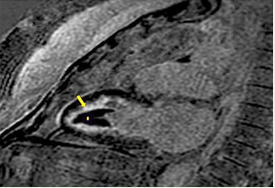
Figure 2a: CMR imaging. Apical 2 chamber, LV endomyocardial edema on T2 weighted images (arrow) and extensive LV mural thrombus with obliteration of the LV cavity (star).
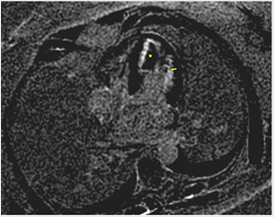
Figure 3a: CMR imaging, Apical 4 chamber, post-contrast late gadolinium enhancement (LGE) images showing extensive subendocardial fibrosis (arrow) and LV mural thrombus (star)
The patient’s hypercoagulable evaluation was unremarkable. There was no etiology for a hypersensitivity reaction. Secondary causes of hypereosinophilia, including parasitic infection, allergic, or pulmonary disease tests were negative. A bone marrow biopsy showed 3% blasts, mildly increased in plasma cells, and normal cellularity which ruled out primary eosinophilic bone marrow disease. C-reactive protein was elevated 1.2 mg/dl. Anti-neutrophil cytoplasmic antibodies test was negative.
Intravenous heparin was started after patient was found to have bilateral PE and LV thrombus. Prednisone 60 mg oral was started for EM. During hospitalization, she developed respiratory distress. She needed high oxygen supply. She was transferred to the intensive care unit. The chest x-ray showed increased interstitial infiltrate of the both lungs. She was started on high-flow oxygen. Chest CT showed significant progression of the infiltrates in her lungs. Her respiratory decompensation was felt to be from eosinophilic pneumonia. She was started on IV pulse steroids, 1 gr methylprednisolone, for three days. Her eosinophilia improved and she responded rapidly. Steroid dose was tapered and she was discharged home on oral steroids and oral anticoagulation.
Discussion
The idiopathic hypereosinophilic syndromes (HES), are characterized by persistently elevated eosinophil count (>1500 eosinophils/mm3), the absence of a primary and secondary cause of eosinophilia, and evidence of eosinophil-mediated end organ damage. [1,2] Cardiac involve ment in idiopathic HES occurs roughly half of the cases [3,4], and is associated with high morbidity and mortality[1,2,5-7].
Echocardiogra phy is the first line diagnostic tool in patients with HES and supported cardiac involvement. As mural fibrosis develops, the LV compliance decreases resulting in a restrictive cardiomyopathy (Figure 1c) [4,8]. Fibrosis also affects the papillary muscle and chordae tendinae resulting in mitral regurgitation, as was observed in this case (Figure 1d)[4,8]. Contrast echocardiography may be invaluable in the diagnosis of LV thrombus and show the shape of the LV to rule out other cause of LV apical obliteration like hypertrophic cardiomyopathy (Figure 1e, Movie 2).
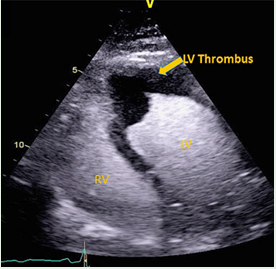
Figure 1e: Apical 4-chamber two-dimensional image with echocontrast at end-diastole showing space-occupying lesion in LV apex due to laminated thrombus
The most distinctive feature of EM on TTE findings is the obliteration of the apex in the left ventricle and right ventricle or both ventricles by laminar thrombus, as was seen here (Movie 1, 2). [3,4,7-9].
CMR is a newer modality for the diagnosis of cardiac disease in patient with HES. [4, 6, 9] CMR can detect ventricular thrombi with a higher sensitivity and specificity than echocardiography, and in addition, contrast-enhanced CMR can identify inflammation and fibrosis[1,4,6,9]. EM is characterized by three sometimes overlapping stages including necrotic, thrombotic, and fibrotic [1,3,5,7]. CMR can provide detailed information about staging of EM which provides additional prognostic information [1,6,9]. CMR can also differentiate EM from other forms of myocarditis, while other forms of myocarditis affect the epicardium and mid myocardial area, EM mostly affect the endocardial and subendocardial myocardium[3].
Our patient had typical TTE findings for EM and CMR provided complementary diagnostic and prognostic information. Historically, endomyocardial biopsy (EMB), has been the ‘gold standard’ for diagnosis of EM[7,10]. EMB has an estimated sensitivity of only 50% and can miss the diagnosis if the area biopsied is not involved[1, 9, 10]. EMB is an invasive procedure and carries risk for iatrogenic complications[1,10]. Moreover, in the absence of right ventricular involvement in our patient per CMR it is quite conceivable that right ventricular EMB would have exposed the patient to increased risk without diagnostic benefit.
EM has roughly 17% in-hospital mortality rate in case series[1]. Early diagnosis and treatment are critical to reduce morbidity and mortality. Secondary causes of HES and primary hematologic diseases should be treated accordingly. Corticosteroids remain the cornerstone of treatment of the different types of HES[4]. In this case, early initiation of high dose steroid controlled progression of the disease, and improved cardiac function. Thrombosis was much more common in EM than one would expect in typical post-viral lymphocytic myocarditis[1,2,7]. Embolic events originating from the intracardiac thrombus are seen in up to 25% of EM cases[2,7]. In our case early initiation of anticoagulation therapy helped to prevent systemic emboli and expansion of PE. While her LV thrombus resolved on the 6 month follow up CMR, she stayed on oral anticoagulation indefinite for unprovoked pulmonary embolism.
Follow-up is an integral part of EM management because some patients can develop a chronic restrictive cardiomyopathy. Serial echocardiogram and CMR are allowing disease monitoring and response to treatment.
During follow-up, the eosinophil counts initially rebounded, necessitating a more prolonged maintenance of low-dose steroid therapy. Follow-up CMR after six months showed normal biventricular function with resolution of LV mural thrombus, decreased subendocardial fibrosis and improved endomyocardial edema (Figure 2b,3b).
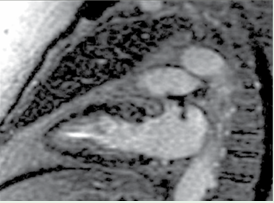
Figure 2b: 6 months follow up CMR imaging. Apical 2 chamber showing resolution of LV thrombus and improvement in myocardial edema.
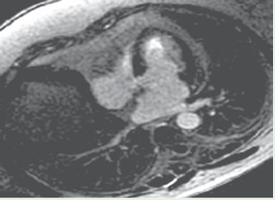
Figure 3b: CMR imaging, Apical 4 chamber, follow-up post-contrast late gadolinium enhancement (LGE) images showing significant improvement of subendocardial fibrosis and resolution of LV mural thrombus
Conclusions
Eosinophilic myocarditis is rare and, in the past, definitive diagnosis has required EMB. In our patient, the diagnosis and decision to proceed with specific therapy were based on a high index of suspicion gleaned from echocardiographic data, supported by confirmatory CMR findings. EMB should be reserved for patients in whom the diagnosis remains uncertain after noninvasive imaging.
Movie
Movie 1: 2D TEE, Apical 4-chamber two-dimensional view showing thrombus obliterating apical LV cavity, extending into mid anterolateral LV wall.
Movie 2: 2D contrast TTE, Apical 4-chamber two-dimensional image with echocontrast shows space-occupying lesion of laminated thrombusin LV apex
How to Cite
References
URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6058919/
URL: https://pubmed.ncbi.nlm.nih.gov/1090795/
URL: https://www.hindawi.com/journals/bmri/2016/2829583/
URL: http://njmonline.nl/getpdf.php?id=1066
URL: https://pubmed.ncbi.nlm.nih.gov/8180373/
URL: https://pubmed.ncbi.nlm.nih.gov/26567231/
URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2048688/
URL: https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1540-8175.2006.00288.x
URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7099847/
URL: https://pubmed.ncbi.nlm.nih.gov/28440714/