Abstract
The present perspective is a synthesis of 171 published investigations comparing the outcomes in patients who underwent hemi-arch or total aortic arch surgeries with deep hypothermic circulatory arrest (DHCA) alone or in conjunction with retrograde cerebral perfusion (RCP), intermittent pressure augmented-retrograde cerebral perfusion (IPA-RCP), antegrade cerebral perfusion (ACP) and total body retrograde
perfusion. In this systematic review we identified 171 investigations addressing the above-mentioned cerebroprotective strategies analysing the role of various neuroprotective techniques for surgeries involving the aortic arch as enunciated above in both experimental and clinical settings.
Studies addressing all cause perioperative mortality, permanent neurological deficits and temporary neurological dysfunction were taken into consideration for identification of the ideal cerebroprotective strategy. Majority of the investigators have preferred different modalities of intraoperative cerebral monitoring.
Keywords
Abbreviations
ALT: Anterolateral Thoracotomy; CBF: Cerebral Blood Flow; CI: Confidence Interval; CPB: Cardiopulmonary Bypass; CT: Computed Tomography; CVA: Cerebrovascular Accidents; DHCA: Deep Hypothermic Circulatory Arrest; EEG: Electro Encephalography; HCA: Hypothermic Circulatory Arrest; SACP: Selective Antegrade Cerebral Perfusion; ICU: Intensive Care Unit; MRI: Magnetic Resonance Imaging; MS: Median Sternotomy; PLT: Poster Lateral Thoracotomy; PND: Permanent Neuro-Deficit; RCP: Retrograde Cerebral Perfusion; SCP: Selective Cerebral Perfusion; TND: Temporary Neurological Dysfunction
Introduction
Surgical treatment of the lesions of transverse aortic arch provides one of the most formidable challenges in aortic surgery [1-14]. The major concern is maintenance of viability of the brain during the period of interruption of cerebral blood flow. Past four decades have witnessed a variety of techniques of maintenance of cerebral integrity during periods of circulatory interruption [1-14]. Because of cerebral auto regulation, there are inherent issues of cerebrovascular spasm, under and over perfusion into an elastic or expansile cerebral vasculature, causing cerebral edema or ecchymosis. Hypothermia has been noted to aggravate the problem when mechanical means of cerebral perfusion were used [1-15]. Recognizing the importance of neuro protection in aortic arch surgeries, deep hypothermic circulatory arrest (DHCA) underpins operative practice as it minimizes cerebral metabolic activity. This facilitates a bloodless operative field and using only DHCA; up to 30 minutes of circulatory arrest can be tolerated [16-18]. For more complex surgeries that require a longer period of circulatory arrest, the adjunctive supplementation of RCP or selective ACP fulfils any lingering cerebral metabolism that has not already been sufficiently moderated by DHCA [19-24].
Retrograde cerebral perfusion in conjunction with DHCA was introduced two decades ago with the aim of reducing cerebral embolism and prolonging “safe duration” of DHCA [25-34]. Studies have demonstrated that retrograde cerebral perfusion enhances the effects of hypothermia. However, its usefulness remains controversial [25-42].
Increased incidence of cerebral edema and intracerebral bleeding has been reported with RCP pressure in excess of 25mmHg [43-47]. Nevertheless, investigators have used even higher RCP pressures in experimental and clinical settings, asserting that the sudden loss of cerebral venous pressure due to conversion from antegrade to retrograde perfusion cause collapse of the cortical veins and increase in resistance of cerebral vasculature [48-51]. Endo, Kubota and associates successfully applied the protocol of intermittent pressure augmented-RCP (IPA-RCP), transiently augmenting the RCP pressure to 45 mmHg using near-infrared oximetry for cerebral monitoring [52,53]. In order to overcome anatomical obstacles due to venous valves at the junction of jugular subclavian vein, Okamoto and associates developed the technique of selective RCP [54]. Experimental studies on brain capillary perfusion during RCP have demonstrated that one-third of arterial oxygen diffuses into surrounding tissues before reaching capillaries and oxygen can also diffuse across venular walls [55-58].
Matanalis and Yasuura have reported the clinical use of bicaval hypothermic retrograde perfusion [20,59-61]. These investigators propose that visceral organs, including the liver and kidneys, can be sustained by oxygenated blood delivered through the systemic venous system at above normal but “safe” venous pressures without deep hypothermia. However the experimental animals demonstrated significant “third space” losses of fluid and little return of blood through the aorta during retrograde perfusion [62].
Over the past 15 years, 10 meta-analyses have reported pairwise comparisons of deep hypothermic circulatory arrest (DHCA), retrograde cerebral perfusion (RCP) and antegrade cerebral perfusion (ACP) in different combinations [64-73]. In 2019, one network meta-analysis (NMA) has compared all three techniques of cerebral protection [74]. Although clinical usefulness of intermittent pressure augmented-retrograde cerebral perfusion, selective RCP, intermittent and continuous RCP, combined retrograde and antegrade cerebral perfusion, and bicaval retrograde perfusion (BIRP) have been demonstrated, the published literature have not taken into consideration these effective modalities of cerebral protection in the meta-analysis. The usefulness of adjunct cerebral perfusion (ACP/RCP/IPA-RCP/BIRP) with longer (>45 minutes) circulatory arrest time and the role of supplementary perfusion in the setting of moderate hypothermia also have not been adequately addressed with statistical model.
Methods
With these deficiencies in mind, we have analysed the published literature to identify the described instances of aortic arch surgery with different techniques of cerebral preservation namely, deep hypothermic circulatory arrest alone or in conjunction with retrograde cerebral perfusion, intermittent pressure augmented-retrograde cerebral perfusion, selective retrograde cerebral perfusion, antegrade cerebral perfusion and total body retrograde perfusion under moderately hypothermic and deep hypothermic circulatory arrest.
The search engines employed were PubMed, Google Scholar, Cochrane Database for Systematic Reviews, Cochrane Central Register of Controlled Trials, Ovid MEDLINE (all; 1946 to 30 10.2019), ACP Journal Club, Ovid EMBASE (1974 to 30.10.2019) and Database of Abstracts of Review of Effectiveness. The search included literature in all languages.
This strategy yielded 171 investigations that provided best answer to these topics. Articles were considered for inclusion if they were adjusted to matched observational studies, or were randomized control trials comparing at least 2 of the 3 cerebral protection strategies.
We included studies that described at least one of the following clinical outcomes: all-cause in-hospital/30 day mortality, permanent neurologic deficits (i.e. presence of new onset permanent neurologic deficits that were focal or global in nature and persisting more than 24 hours according to STS definition), morbidity of transient neurologic dysfunction. Transient neurological dysfunction (TND) is defined as postoperative confusion, agitation, delirium, transient parkinsonism or prolonged obtundation) and stroke (defined as a serious illness caused by blockage or rupture of an intracranial vessel), diagnosed by computed tomography or magnetic resonance imaging and composite 30-day / in-hospital major morbidity [defined by STS as any reoperation, prolonged (>24 hours) ventilation, acute renal failure (maximum postoperative creatinine 2 x the baseline creatinine and >2.0 g/dl) and new onset dialysis].
Conference presentations, expert opinions, editorials, studies not defining the strategy used or using multiple cerebral protection strategies simultaneously and studies not defining or reporting postoperative stroke or operative mortality outcomes for individual cerebral perfusion strategies were excluded. Manual searches of reference lists did not identify any other relevant studies.
With respect to drawing conclusions from the literature, we have synthesized all available data in this systematic review to outline the rationale, issue of concern, and potential future trends of various strategies of cerebral protection during reconstruction of the aortic arch with or without reimplantation of the arch vessels. We assessed the publication bias by using Forest plots. All analyses were done with STATA Software (version 12, Statacorp. LP, College Station, Texas, USA).
Concept
Strategies for cerebral protection during surgeries for aortic arch have evolved into three categories: deep hypothermic circulatory arrest, selective antegrade cerebral perfusion and retrograde cerebral perfusion. Hypothermic circulatory arrest (HCA) is a well-established method to confer cerebral protection during operations involving the aortic arch with interrupted antegrade flow [75-79]. DHCA avoids the use of aortic clamp and consequently provides a bloodless operative field, uncluttered with instruments and allows more meticulous arch reconstruction [75-79]. During DHCA, protection of the brain, heart, kidneys and other organs is achieved by reducing metabolic activity.
This strategy, however, sets time constraints on the operation and is still associated with significant neurologic morbidity. During DHCA, brain metabolism is not completely halted but continues in an ischemic environment. This exposes the brain to hypoxia, hypercapnia, acidosis, and elevated levels of excitotoxins that may cause neuronal apoptosis and necrosis. Additionally it requires prolonged cooling and rewarming time and results in subsequent coagulopathy [80-83].
Cumulative evidence in the published literature have demonstrated dramatic rise of neurological dysfunction beyond 40 to 45 minutes of ischemic interval and marked increase in mortality rate beyond 65 minutes of circulatory arrest [81].
In 1986, Frist and colleagues revived the concept of antegrade cerebral perfusion (ACP) under moderate hypothermia with 90% survival after arch replacement using unilateral ACP [84]. Selective ACP is a useful adjunct when reconstruction of the aortic arch and arch vessels is likely to take a long time. However, antegrade cerebral perfusion requires complicated cannulation techniques and increases the clutter in the operative field. The procedure also increases the risk of particulate embolization secondary to cannulation-induced dislodgement of atheromatous debris [19-24,83,85].
Mills and Ochsner first clinically employed retrograde cerebral perfusion, as a treatment of massive air embolism during cardiopulmonary bypass in 1980 [86]. In 1982, Lemole and associates reported the use of intermittent RCP during repair of dissected thoracic aorta implanting an intraluminal suture less prosthesis [87]. In 1982, Ueda and associates introduced intermittent and continuous RCP to extend the safe duration of DHCA during surgical treatment of aortic arch aneurysm [88].
Retrograde cerebral perfusion (RCP) through the superior vena cava during DHCA has been introduced to improve cerebral protection during this vulnerable period. It has been proposed that RCP may increase cerebral ischemic tolerance and prolong the clinically safe duration of circulatory arrest by providing metabolic support, catabolite removal, washout of gaseous and particulate emboli, and preventing brain rewarming during the arrest period [25-32]. In addition, the operative field is unencumbered by additional cannulas or clamps and there is no requirement of invasion of the cerebral vessels, thus mitigating the risk of atheromatous particulate embolization [89-92].
Between 2000-2003, studies have focussed on brain capillary perfusion during retrograde cerebral perfusion [41,42,55,56]. Antegrade micro-circulation studies suggest that capillary bed perfusion may not be essential for oxygen exchange because a substantial amount of arterial oxygen (one-third) diffused into the surrounding tissue before blood reaches the capillaries and oxygen can also diffuse across the venular walls [57,58]. However, the extent of oxygen carrying capacity and diffusion from retrogradely perfused blood towards aerobic metabolic support is unknown.
Moderate hypothermia with cold retrograde cerebral perfusion at 10°C have been successfully introduced in clinical practice for surgical treatment of acute type A aortic dissections and aortic arch replacements [93,94]. Moshkovitz and colleagues in Toronto used cold retrograde cerebral perfusion at 10°C during moderately hypothermic (22-26°C) circulatory arrest demonstrating the safety of this method for up to 30 min of hypothermic circulatory arrest [95]. They reported excellent outcomes of this techniques used in 104 patients operated on for disease of the proximal aorta.
To overcome the ischemic neurologic events beyond 60 min of circulatory arrest, Yasuura, Matalanis and Buxton developed a technique of retrograde bicaval perfusion to protect the brain and other systemic organs [20,59-61]. They used this technique in 34 patients undergoing surgeries on the aortic arch. Good cerebral protection had been obtained by this method in most patients, including 2 patients with RCP exceeding 100 min. In 19 patients, the RCP was performed through conventional vena caval cannulas.The occurrence of serious neurological injury in one patient raised concerns of the venous valves at the jugular-subclavian junction, impeding retrograde flow to the brain.
In 1988, Midy and associates demonstrated the presence of venous valves at the junction of jugular and subclavian vein in 80% to 90% of humans [96]. Most of these valves are vestigial and incompetent, but in 10%-20% of patients, these valves are competent and may interfere with retrograde flow through the superior vena cava (SVC) to the brain. Since there are no valves in the internal jugular vein above the venous angle as well as in the intracranial sinuses, Okamoto and associates developed a safe technique of selective jugular venous cannulation (24F or 26F) through the right atrium using a central venous catheter (7F or 8F). Between 1991 and 1993, these investigators successfully used this technique in 15 consecutive patients undergoing aortic arch surgeries and concluded that this technique may provide more effective cerebral protection than simple retrograde cerebral perfusion through the SVC [54].
Surgical Techniques and Management
Surgical management has evolved with time. Depending on the institutional protocol and the preference of the surgeon diverse strategies of cerebral protection have been employed.
Cerebral monitoring
Several modalities are used to evaluate cerebral perfusion during aortic arch surgery. The techniques include preoperative computed tomographic angiography of the brain, right radial, superficial temporal arterial pressure line, jugular venous oxygen saturation, near-infrared spectroscopy (NIRS) cerebral monitoring, intermittent transcranial echo Doppler, laser speckle flow graphic assessment of microcirculation of the optic nerve head, intraoperative electroencephalography, and retrograde cerebral perfusion pressure monitoring.
Temperature
The data from the published literature indicated that the majority of centres rely on some level of hypothermic perfusion with the average of perfusate temperature being 22°C. Support for moderate hypothermia has been confirmed in experimental and clinical settings in which no advantage was found to drop the temperature below 25°C [97-102].
Published literature documents the following surgical options to perfuse cerebral tissue, thus prolong the safe period of hypothermic cerebral ischemia.
pH-stat vs α-stat management during hypothermic cardiopulmonary bypass
The management of pH during CPB has been extensively investigated but remains controversial. Although α-stat blood gas management during hypothermic CPB is widely used, particularly in adult patients, pH-stat management is more physiological, and used more commonly in children [75-79]. Use of a pH-stat strategy during hypothermia has been reported to: i) decrease cerebral metabolism;[103-105] ii) increase cerebral blood flow; [106-110] and iii) increase the rate of brain cooling [9], and counteract the hypothermia induced leftward shift of the oxyhemoglobin dissociation curve, thereby enhancing oxygen availability [111]. However, the α-stat strategy has been extensively used in the published literature for blood pH measurement during RCP in both experimental and clinical settings [103,105,107-109].
Selective antegrade cerebral perfusion
Patients undergoing moderate hypothermic circulatory arrest with antegrade cerebral perfusion are usually cooled to a nasopharyngeal temperature of 20°C to 26°C. At the initiation of circulatory arrest, ACP through brachiocephalic artery and left common carotid artery is initiated between 10-15 ml/kg/min to maintain the cerebral arterial pressure between 50-60 mmHg monitored by a right radial arterial line.
Sabik and associates recommended axillary artery cannulation technique for antegrade aortic perfusion [112].Various investigators including ourselves have used right brachiocephalic artery and left common carotid artery perfusion for ACP during transverses aortic arch aneurysm surgeries [18,98,99,113-115]. Antegrade cerebral perfusion can be achieved by direct cannulation or by anastomosing a side graft to the right axillary artery, left carotid artery or brachiocephalic artery. Alternatively, the brachiocephalic artery can be accessed, in order to avoid the risks of brachial plexus injury by axillary artery inflow [113-115].
Occlusion / clamping of the distal aortic arch with selective ACP using brachiocephalic, left common carotid or left subclavian arteries may cause crowding and distortion of the aortic lumen. The fragile, dissected aortic intimal flap too often resulted in fragmentation of the fragile aortic wall and further aortic dissection on resumption of the aortic flow [18,98,99,113-115].
Conventional retrograde cerebral perfusion
Adjunct retrograde cerebral perfusion through a SVC cannula may extend the duration of safe cerebral circulatory arrest. Deep hypothermic cerebral perfusion lowers the brain temperature and lessens the risk of cerebral injury by reducing blood cell micro aggregation, providing nutrients and back washing of air bubbles, toxic metabolites and embolic debris [43-47]. Following hypothermic circulatory arrest, RCP is initiated via SVC cannula and maintained at a flow rate of 100-300 ml/min to maintain perfusion pressure between 15-20mmHg to avoid cerebral edema and ecchymosis.
Retrograde cerebral perfusion with intermittent pressure augmentation
Kitaheri & colleagues and Kawata & colleagues from Japan developed this novel protocol of retrograde cerebral perfusion, i.e., intermittent pressure augmented retrograde cerebral perfusion (IPA-RCP) elevating the SVC perfusion pressure to 45 mmHg every 30 seconds in a canine model [49-51]. During DHCA, adjunct RCP is normally administered at a pressure between 15 and 20 mmHg to avoid cerebral edema. However, the duration of safe prolongation of DHCA is limited, because at these pressures the intracranial vessels do not fully open.
In 2010, Kubota and associates in collaboration with above investigators employed this technique of IPA-RCP in a 25-year-old female with aortitis syndrome with completely occluded brachiocephalic and left subclavian artery. The right hemisphere
was perfused by the left internal carotid artery through the circle of Willis with an aneurysm extending from the ascending aorta to the aortic arch, having a maximum diameter of 76mm, and severe aortic regurgitation. The patient successfully underwent isolated bio prosthetic aortic valve replacement with synthetic graft replacement of the ascending aorta and total arch with re-implantation of the brachiocephalic artery and left common carotid artery [53].
These authors perfused oxygenated blood at pressure of 15-20 mmHg for 2 minutes followed by augmented perfusion of 45 mmHg for 30 seconds. This sequence was repeated through the arch reconstruction. Postoperatively recovery was uneventful with no neurological deficit and improved right brain perfusion [53].
Selective jugular cannulation for retrograde cerebral perfusion
Because there are no valves in the internal jugular vein above the venous angle as well as in the intracranial sinuses, Okamoto and associates developed a technique of selective cannulation of the internal jugular vein [54]. Selective jugular cannulation is performed by the “reversed over-the-wire cannulation” technique as described under:
At the induction of anaesthesia a 7F or 8F central venous catheter is inserted through the internal jugular vein into the right atrium (RA). Total cardiopulmonary bypass (CPB) is established with bicaval venous cannulation through the RA and common femoral arterial cannulation. Myocardial protection is achieved using retrograde coronary sinus perfusion of cold blood cardioplegia. Systemic cooling is continued till rectal temperature of 20°C. Proximal aortic repair is performed during this period of cooling [54].
At this point, the CPB is temporarily discontinued, the SVC cannula is removed, and both venae cavae are snared. A short right atriotomy is performed and a 0.35 inch guidewire through a 24F or 26F venous cannula is inserted into the central venous catheter tip. The SVC cannula is advanced retrogradely over the central venous catheter into the internal jugular vein beyond the venous valve at the venous angle. Next, the guide wire is pulled out by the anaesthesiologist and the SVC cannula is connected to the CPB circuit. The aortic cross clamp is removed and retrograde perfusion is initiated; open distal anastomosis is then performed [54].
Intermittent retrograde cerebral perfusion
In 1988, Kusuhara and colleagues successfully employed intermittent retrograde cerebral perfusion through SVC under profound hypothermic circulatory arrest for surgical treatment of aortic arch aneurysm [116].
Total body retrograde perfusion
The use of the “open” distal anastomosis technique has permitted satisfactory results of aortic arch reconstruction [10]. An “open” distal anastomosis during circulatory arrest simplifies the procedure, avoids clamp injury to the fragile dissected aortic tissue, and allows direct visualization of lesions involving the aortic arch and its tributaries. The optimal level of hypothermia and its effectiveness in achieving cerebral and visceral protection during circulatory arrest is unknown.
Yasuura K and associates developed a technique of hypothermic total body retrograde perfusion to achieve systemic organ protection: cerebral protection by continuous retrograde perfusion of the SVC, myocardial protection by retrograde coronary sinus infusion, and abdominal visceral organ perfusion by continuous retrograde perfusion through the inferior vena cava (IVC) [59-61].
Hendrik S and associates suggested that retrograde perfusion through the vena cava might maintain normal aerobicity of vital organs [117]. As retrograde perfusion is not a physiologic circulation, some investigators have attempted to determine the amount of actual nutritive blood flow provided by retrograde perfusion. They demonstrated that retrograde SVC perfusion provided half of cerebral blood flow and retrograde IVC perfusion provided about a third of hepatic and renal blood flow [45-47]. Although organ blood flow increased at high perfusion pressures, ascites developed and circulating blood volume decreased.
Portal venous pressures varied proportionally with IVC pressure, and high portal venous pressures led to increased mesenteric vascular permeability and production of ascites. It has been reported that ascites will accumulate at portal venous pressures greater than 17.5 mm Hg. Based on Starling’s law, ascites production would be expected above a capillary pressure of 25 mm Hg. The authors added retrograde IVC perfusion to retrograde SVC perfusion for abdominal organ protection in patients undergoing aortic arch operations. Retrograde IVC perfusion increased blood supply to the abdominal organs; however, it also was associated with ascites production. They recommended maintenance of IVC perfusion pressure of less than 25 mmHg to prevent ascites.
During retrograde perfusion, venous valves may disturb blood flow. Immature venous valves are present at the venous angle in 7.8% of Japanese [118]. However, no venous valves exist in the IVC. In Japanese, venous valves are present at the hepatic venous junction in 1.6%, and none were observed at the renal venous junction [119]. Therefore, the presence of venous valves is inconsequential in retrograde IVC perfusion [119].
Results
The overall operative mortality and risk of cerebrovascular accidents for patients undergoing surgeries of the aortic arch using DHCA with and without antegrade or retrograde cerebral perfusion is 6% to 23% and 2% to 12% respectively among various centres practicing surgeries of the aortic arch. These patients died of diverse causes, including low cardiac output syndrome, cerebrovascular accidents, bleeding diathesis, renal failure requiring dialysis, pulmonary infection, hepatic failure and coagulopathy (Tables 1-7) [13,64-74].
Table 1: Summary of the published clinical investigations documenting the mortality and morbidity following deep hypothermic circulatory arrest and retrograde cerebral perfusion or deep hypothermic circulatory arrest and antegrade cerebral perfusion
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables |
Mortality |
Morbidity |
Conclusions |
|
1. |
Ueda Y et al, 1994 [88] |
DHCA+RCP, n=33 |
Replacement of the ascending aorta or aortic arch, intermittent and continuous RCP to extend the safe duration of HCA during arch surgeries |
In-hospital 30 days (6%) |
Stroke 6% |
RCP is a useful adjunct to DHCA upto 80 minutes to perfusion |
|
2. |
Raskin SA, 1995 [91] |
DHCA+RCP, n=88 |
Replacement of the ascending aorta or aortic arch Mean age: 63 years (range 28-78 years) Mean circulatory arrest time: 31 minutes (range 10-62 minutes) Lowest nasopharyngeal temperature: 14°C Cerebral flow-pressure: 25mmHg (upper limit) |
In-hospital 2 (2%) |
Stroke No postoperative strokes |
RCP during DHCA decreased the surgical and neurological morbidity, and has the potential for reduction of embolization of air and atheromatous debris |
|
3. |
Usui A et al, 1996 [43] |
DHCA+RCP, n=228 |
Replacement of the ascending aorta or aortic arch |
In-hospital 6.1% 30 days 13.6% |
Neurologic dysfunction: 20% |
Perfusion pressure >25 mmHg – increased incidence of cerebral edema and intracerebral bleeding |
|
4. |
Okita Y et al, 1998 [36] |
DHCA+RCP, n=50 DHCA+SACP, n=253 DHCA, n=50 CPB, n=297 |
Replacement of the ascending aorta or aortic arch |
In-hospital 6% 19% 12% 13.8% |
Cerebral complications 4% 18% 8% 3.7% |
Method cerebral perfusion did not influence outcome |
|
5. |
Bavaria JE et al, 1995 [33] |
DHCA+RCP, n=19 DHCA, n=20 CPB, n=21 |
Replacement of the ascending aorta or aortic arch |
60 day 5% 40% 19% |
CT/MRI- confirmed CVA 0% 33% 20% |
RCP resulted in less mortality than HCA. RCP resulted in fewer strokes than HCA and CPB |
|
6. |
Coselli JS and LeMaire SA, 1997 [30] |
DHCA+RCP, n-290 DHCA, n-189 |
Replacement of the ascending aorta or aortic arch |
In-hospital 30 day 3.4% 2.4% 16.9% 14.8% |
Stroke 2.4% 6.5% |
RCP resulted in less mortality and fewer strokes than HCA |
|
7. |
Coselli JS, 1997 [31] |
DHCA+RCP, n=305 DHCA, n=204 |
Replacement of the ascending aorta or aortic arch |
In-hospital 3.9% 17.16% |
Stroke 2.62% 6.37% |
RCP resulted in less mortality and fewer strokes than HCA |
|
8. |
Safi H et al, 1997 [25] |
DHCA+RCP, n=120 HCA, n=41 |
Replacement of the ascending aorta or aortic arch |
Nil |
CT/MRI-confirmed stroke 2.5% 9.8% |
RCP resulted in significantly fewer strokes than HCA |
|
9. |
Moshkovitz Y et al, 1998-95 |
Moderate HCA+RCP at 10°C, n=104 |
Replacement of the ascending aorta or aortic arch, moderate HCA (22-26°C, RCP at 10°C) |
In-hospital 7.7% |
Stroke 7.7% Seizures 3.8% |
Combination of moderate HCA with RCP at 10°C- safe upto 30 minutes of HCA |
|
10. |
Ehrlich M et al, 1998 [41] |
DHCA+RCP, n=28 DHCA, n=65 |
Replacement of the ascending aorta or aortic arch |
30 day 14% 40$ |
Neurological dysfunction 10% 21% |
RCP resulted in less mortality and neurological dysfunction than HCA |
|
11. |
Usui A et al, 2012 [162] |
DHCA+RCP, n=75 SACP, n=91 |
Replacement of the ascending aorta or aortic arch |
In-hospital 24% 21% |
Neurologic dysfunction 16% 19% |
No difference between RCP and SCP in death or neurologic dysfunction |
|
12 |
Okita Y et al, 2001 [37] |
DHCA+RCP, n=76 DHCA+SACP, n=112 Partial CPB, n=58 |
Replacement of the ascending aorta or aortic arch |
In-hospital Late 8% 4% 23% 3% 21% 28% |
Stroke 4% 11% 24% |
Method of cerebral perfusion did not influence outcome |
|
13. |
Moon MR et al, 2002 [139] |
DHCA alone, n=36 DHCA+RCP, n=36 |
Study period 1996-2000 Lowest core temperature — 18°C±2°C (12-24°C) DHCA: 19.5±2.3 DHCA+RCP: 19.2±3.2 p=0.64 |
In-hospital 8.1±5% 11±5% p>0.95 |
Neurological deficits 14%±6% 14%±6% p>0.73 |
Supplmental RCP during HCA did not decrease mortality or neurologic complications. Retrograde rewarming through femoral artery increased transient neurological dysfunction. RCP remains optional. Reperfusion should be antegrade |
|
14. |
Yamashita C et al, 1998 [35] |
38 patients |
Study period: 1986-1996 Distal aortic arch aneurysm, Group I- graft anastomosis with ACC and left heart bypass (1986-89), MS+ALT= 9, PLT=7 Group II: MS+ALT, open anastomosis, graft anastomosis, RCP, DHCA Group III- open anastomosis with RCP in Trendelenburg position, PLT |
Hospital death Group I: 25% (4/16), died of stroke, MI Group II: 37.5% (3/8), respiratory failure, aortic dissection Group III: 7.1% (1/14), congestive cardiac failure |
Nil |
RCP with a posterolateral thoracotomy minimizes the risk of stroke and respiratory failure during arch operation |
|
15. |
Tonoue Y et al, 1999 [28] |
RCP, n=15 ACP, n=17 |
Study period: 1993-1997 Lowest nasopharyngeal temperature: 15.9°C Perfusion time (min): RCP (38.3±1.46); ACP (71.9±40.4) Pump flow rate (ml/min): RCP (459±270); ACP (500) Perfusion pressure (mmHg): RCP (22.7±4.0); ACP (35.1±12.5) Tympanic membrane (°C): RCP (16.7±2.2); ACP (15.9±3.5) |
RCP, n=2 (stroke) SCP, n=1 (bleeding) |
SCP stroke, n=3 |
The measurement on middle cerebral artery blood flow velocities with transcranial doppler is practicable during SC, difficult during RCP indicating critical decrease in CBF during RCP |
|
16. |
Coselli JS, 1994 [32] |
DHCA+RCP, n=88 |
Study period: 1992-93 Arch repair – DHCA circulatory arrest CPB time-113 (range 66-216 minutes), circulatory arrest 31 (10-62 minutes), EEG- isoelectric at nasopharyngeal temperature 72°C to 25.4°C |
30 days mortality, n=2 |
No postoperative stroke |
Clinically safe method ◻ DHCA+RCP |
|
17. |
Okamoto H et al, 1993 [54] |
RCP (conventional), n=19 RCP (selective), n=34 |
Aortic arch operation |
RCP (conventional), n=1 RCP (selective)- no event including 2 patients with RCP >100 minutes |
Nil |
10-20% patients have functioning venous valves at jugular-subclavian junction which may interfere with RCP. Satisfactory cerebral protection should be possible with selective RCP >60 min |
|
18. |
Bonser RS et al, 1999 [39] |
DHCA. n=21 DHCA+RCP, n=21 |
Lowest NP temperature: 15°C SVC perfusion: 25 mmHg, transcranial paired arterial and jugular bulb blood: oxygen, glucose HCA duration min (mean±SD): HCA (32±9); RCP (27±12.3); p=0.14 RCP duration min (mean±SD): (23±9.6) CPB duration min (mean±SD): HCA (145±24.3); RCP (153±35.7), p=0.4 Ascending aortic + aortic root resection: HCA (n=13), RCP (n=13) Hemiarch± root: HCA (n=3), RCP (n=3) Total arch± root: HCA (n=3), RCP (n=3) |
Hospital death DHCA, n=1 RCP, n=2 Permanent neurological deficit DHCA, n=1 RCP, n=0 Transient neurological deficit DHCA, n=0 RCP, n=2 |
Nil |
Transcranial oxygen extraction during RCP 3.3 ml/dl, range 0.7- 6.6 ml/dl, significantly higher than extraction with antegrade perfusion before and after HCA (p<0.1), RCP flow was insufficient to maintain cerebral oxygenation, RCP may improve cerebral protection through other mechanism |
|
19. |
Lau C et al, 2018 [134] |
1043 patients |
Study period: 1997-2014 Age mean: 65.7±13.3 years, DHCA + RCP perfusion time >50 minutes <49 minutes P value Number 50 993 Age (years) 61.2±13.4 65.9±13.3 0.014 |
Mortality group >50 min versus 49 min, 8% vs 3.8% (p=0.14), stroke rate 2% vs 1.2% (p=0.62), propensity matching resulted in 48 pairs. DHCA duration was not independently associated with operative death or postoperative neuro deficits. RCP- effective adjunctive cerebral protection strategy for aortic arch aneurysm surgeries, not associated with increased death or neurological complications |
||
|
20. |
Wong CH and Bosner RS, 1999 [45] |
DHCA, n=34 DHCA+RCP, n=96 |
Study period 1991-1998 Age: 2-=84 years (mean 62.7 years) Emergent surgery 46/130 (35.4%), lowest temperature 15°C, alpha stat pH DHCA- arrest duration 30.1 min (2-80 minutes) , p<0.019 DHCA+ RCP- circulatory arrest 24.4 (8-53 minutes), p<0.019 Multivariate logistic regression- RCP duration (p<0.038) as risk factors for mortality, and myocardial ischemic time (0.012) ahd HCA duration (p=0.05) as risk factor for stroke. HCA and RCP groups differed in HCA duration (HCA mean 25 min (10-80), RCP mean 32 min (10-69), p<0.019 Mortality: DHCA+RCP (15%), Stroke (7%) DHCA alone (24%), Stroke (6%) |
Age and HCA remain risk factors for stroke and mortality despite RCP, HCA times were longer in the RCP patients, patients were not randomized |
||
|
21. |
Esmailian F et al, 1999 [32] |
52 patients |
Study period: 1991-1998 Age 3 weeks-89 years, mean RCP time 39.5 minutes (3-88 minutes), RCP >45 min, n=16 (31%) Core temperature 19.3 (15-27°C), RCP >45 min, n=12 - no. CVA, RCP >70 min, n=2- major CVA-died, subdural hematoma, n=1 Temporary mental abnormality, normal CT |
RCP-reliable and technically appealing, removed air, particulate matter |
||
|
22. |
Ganapati AM et al, 2014 [71] |
DHCA+ACP, n=360 DHCA+RCP. N=80 Propensity matched ACP, n=40 RCP, n=40 |
Study period: 2005-2013 Propensity matched analysis – DHCA+ACP vs DHCA + RCP – hemi arch replacement, a propensity score with 1:1 matching of 40 pre and intraoperative variables used to adjust for differences between groups Between ACP and RCP- no differences in 30 day/in-hospital mortality or morbidity outcomes, total arch cases were excluded to limit the analysis to shorter DHCA times and a more uniform patient population |
In proximal arch operations using DHCA, equivalent early and late outcomes can be achieved with RCP and AC |
||
|
23. |
Hu Z et al, 2014 [70] |
DHCA+ACP, n=2855 DHCA+RCP, n=1897 |
15 studies; pooled analysis- no difference in 30 day mortality, PND & PND in the 2 groups |
ACP and RCP provide similar protective effectiveness combined with DHCA and could be selected according to the actual condition in aortic arch surgery |
||
|
24. |
Guo S et al, 2015 [66] |
DHCA+ACP, n=4262 DHCA+RCP, n=2761 |
Meta-analysis of 34 studies TND-risk ratio 0.72 (95% CI 0.58-0.90); Z score 2.9, p=0.004 Patients undergoing DHCA+ACP- better outcomes in terms of TND compared to DHCA+RCP No difference between group in terms of PND, stroke and early mortality |
DHCA+ACP has an advantage over DHCA+RCP in terms of TND, while the two methods show similar results in terms of PND, early mortality and stroke |
||
|
25. |
Okita Y et al, 2015 [115] |
ACP, n=7038 HCA+RCP, n=114 |
Study period: 2009-2012 Total arch replacements, n=16218 ACP vs HCA+RCP, analysis on 8169 patients (ascending aortic dissection, ruptured aneurysm, emergency surgery – excluded) 30 day mortality 3.2% vs 4.0%, hospital death 6.0% vs 7.1%, stroke 6.7% vs 8.6%, TND 4.1% vs 4.4%, no difference in composite outcome of hospital death, stroke, need for dialysis, prolonged ICU stay > 8 days 24.2% vs 15.6% with HCA/RCP |
Both techniques provide comparable clinical outcomes with regard to mortality, stroke rate. HCA/RCP – prolonged ICU stay |
||
|
26. |
Tian DH et al, 2018 [65] |
HCA, n=2705 HCA+RCP, n=2817 |
Twenty-eight comparative studies that included patient groups undergoing aortic arch surgery using HCA or HCA+RCP Significantly increased mortality – DHCA compared to DHCA + RCP, odds ratio 1.75, 95% CI: 1.16-2.63, p=0.007, I2 54%; stroke significant increase in HCA group (OR 1.5, 95% CI: 1.07-2.90, p=0.02), I2 29%; temporary neurodeficits- no difference (p=0.66) |
Addition of RCP may provide better outcomes than using HCA alone |
||
|
27. |
Hameed I et al, 2019 [74] |
ACP, n=15293 RCP, n=7511 DHCA, n=4164 |
68 studies, n=26968 patients; USA, n=19; Japan, n=13; Germany, n=6; other countries, n=30 6 randomized controlled trials (n=354), 62 observational studies (n=26,614), Mean age: ACP 48.1-71 years, RCP 48.5-71 years, DHCA 49-68.1 years; compared with DHCA, both ACP and RCP were associated with significantly lower postoperative stroke and operative mortality rates, ACP odds ratio 0.62 (95% CI: 0.51-0.75) odds ratio 0.66 (95% CI: 0.51- 0.76) respectively RCP odds ratio 0.66 (95% CI: 0.54-0.82), odds ratio 0.57 (95% CI: 0.45-0.71) respectively; ACP and RCP associated with similar incidence of primary outcome; relative benefit increases with the duration of circulatory arrest. |
No difference among 3 techniques on secondary outcome. Unilateral or bilateral antegrade cerebral perfusion did not influence the results, when arrest time exceeded 25 min- the benefits of RCP, ACP over DHCA become significant |
||
|
28. |
Ganzel, BL et al 1997 [132] |
Study period: 1993-1996 Complex aortic and aortic arch surgeries- neurophysiologic monitoring DHCA+RCP, n=22 DHCA alone, n=8 Circulatory arrest duration (min) 26 (22-30) 24 (15-33) Temperature °C 17 (16-19) 17 (14-20) Decrease of regional cerebral venous oxygen saturation |
Under the guidance of multimodality neurologic monitoring, high flow RCP as safe as circulatory arrest alone |
|||
|
29. |
Tian DH et al, 2013 [64] |
Aortic arch operation, meta-analysis of 9 studies, DHCA alone n=64.8, DHCA+SACP n=370; DHCA+SACP was associated with superior survival outcomes (p=0.008), i2=0%. No difference in permanent neurologic outcomes |
DHCA+SACP was superior to DHCA alone |
|||
|
30. |
Okita Y et al, 2001 [37] |
Study period: 1997-1999, total aortic arch replacement; DHCA+RCP, n=30; DHCA+SACP=30 Hospital death: RCP (6.6%; SCP (6.6%) New strokes: RCP (3.3%), SCP (6.6%), p=0.6 TND: RCP (33.3%), SCP 13.(3%), p=0.05 |
Both methods of cerebral protection resulted in acceptable morbidity and mortality. The prevalence of TND was significant higher in RCP |
|||
|
31. |
Gatti G et al, 2017 [150] |
Study period: 1999-2015; aortic arch operation DHCA 14-20°; DHCA+RCP=344, DHCA alone= 26 (control group), in hospital death (9.6%), PND (9%), TND (19.1%) |
DHCA+RCP- low risk of TND provided DHCA 25 min |
|||
Table 2: Summary of the published clinical investigations documenting the mortality and morbidity following deep hypothermic circulatory arrest + retrograde cerebral perfusion, moderately hypothermic circulatory arrest and antegrade cerebral perfusion
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables, mortality, morbidity and statistical significance |
Conclusions |
|
1. |
Milewski RK et al, 2010154 |
DHCA+RCP, n=682 MHCA+ACP, n=94 |
Study period: 1997-2008 Analysis of two institutions; mean cerebral ischemic time and visceral ischemic time differed between RCP/DHCA and ACP/MHCA (p<0.001). There was no significant difference in permanent neurologic, deficit, temporary neurologic dysfunction, or renal failure, between RCP/DHCA and ACP/MHCA on multivariate analysis. Mortality was comparable across both techniques |
Both techniques have emerged as effective techniques for selected aortic arch operations with low morbidity and mortality, no statistically significant difference in primary or secondary outcomes between techniques for aortic reconstruction times less than 45 minutes |
|
Study period: 2006-2014 |
MHCA/ACP was associated with 76.5% decreased risk (RR 0.23, 95% CI: 0.07 to 0.69) of postoperative neurologic complications (p=0.009), mid-term all cause mortality MHCA/ ACP modestly decreased the number of deaths (p=0.04), MHCA/ACP- a trend towards decreased 30 day and mid-term mortality |
|||
|
Propensity score matching analysis of 259 patients, after propensity scoring 40 pairs (80 patients) matched |
||||
|
Before matching |
||||
|
2. |
Perreas K et al, 2016163 |
Ascending aortic + hemiarch correction, n=259 DHCA/RCP, n=207 |
After matching |
|
|
MHCA/ACP. n=52 |
DHCA/ RCP |
|||
|
MHCA/ ACP |
||||
|
P value |
||||
|
DHCA/ RCP |
||||
|
MHCA/ ACP |
||||
|
P value |
||||
|
3. |
Leshnower BG et al, 2019102 |
DHCA+RCP, n=11 MHCA+ACP, n=9 |
Hemiarch replacement, nasopharyngeal temperature Stroke p value DHCA+RCP 19.9°±0.1°C (p<0.0001) 5/11 (45%) 0.01 MHCA+ACP 26.3°±1.8°C 9/9 (100%) Mortality / renal failure – Nil |
MHCA + ACP may be associated with a higher incidence of radiographic neurologic injury than DHCA + RCP in patients undergoing hemiarch replacement |
ACP-antegrade cerebral perfusion, CI-confidence interval, DHCA-deep hypothermic circulatory arrest, MHCA-moderate hypothermic circulatory arrest, RCP-retrograde cerebral perfusion,
Table 3: Summary of the published clinical investigations documenting the mortality and morbidity following deep hypothermic circulatory arrest and intermittent pressure augmented retrograde cerebral perfusion
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables, mortality, morbidity and statistical significance |
Conclusions |
|
1. |
Kubota H et al, 201053 |
25 years female |
Diagnosis aortitis with ascending aortic arch aneurysm, CT-aneurysm from ascending aorta to aortic arch, maximum diameter 76 mm, MR angio- occlusion- BCA, LSA, right brain perfused via LICA, Echo-severe AR, bioprosthetic AVR: 21mm, total ascending aortic and arch replacement, reimplantation- BCA, LCCA, lowest temperature: 18°C, circulatory arrest, IPA-RCP, SVC pressure 15-20 mmHg x 2 min, 45 mmHg x 30 seconds, repeated every 20 minutes, duration- IPA-RCP: 75 minutes, RSO2 maintained: 80-85%, postoperative brain perfusion scintigraphy-improved perfusion- right cerebral hemisphere |
IPA-RCP may contribute to brain protection and better clinical outcomes |
|
2. |
Endo H et al, 201352 |
DHCA-CRCP, n=10 DHCA-IPA-RCP, n=10 |
Study period: 2005-2008 DHCA-CRCP – continuous venous pressure 25mmHg DHCA-IPA-RCP – venous pressure 20mmHg (120 seconds), 45 mmHg (30 seconds) rSO2- near infraread spectroscopy every 10 min Mortality- Nil, major neurological complications – nil Full wakefulness – end of surgery to fully awake- conventional RCP 310±282 min, IPA-RCP 85±64 min (p<0.5) rSO2 greater than conventional RCP from 10-70 mmHg (p<0.5) |
IPA-RCP provides more homogenous cerebral perfusion and a more effective supply |
AR-aortic regurgitation, AVR-aortic valve replacement, BCA-brachiocephalic artery, CT-computed tomography, IPA-RCP- intermittent pressure augmented retrograde cerebral perfusion, LCCA-left common carotid artery, LICA-left internal carotid artery, LSA-left subclavian artery, RSO2-cerebral arterial oxygen saturation, SVC superior vena cava
Table 4: Summary of the published clinical investigations documenting the mortality and morbidity following deep hypothermic circulatory arrest and retrograde coronary sinus and retrograde superior and inferior vena caval perfusion
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables |
Mortality |
Morbidity |
Conclusions |
|
1. |
Yasuura K et al, 199259 |
5 patients |
Study period: 1990-1991 Age: 18-59 years, Median: 54 years, ascending aortic replacement±Bentall, CPB mean time: 253 (range 162-351 minutes), rectal temperature during RCP: 16-20°C, mean time total RCP: 82 minutes (range 32-110 minutes) |
Nil |
No neurological complications, postoperative BUN: 28-30 mg/dl, serum creatining 1.5-1.8 mg/ dl, LFT-normal |
Total body retrograde perfusion creates a relatively bloodless field, permits complete repair without fear of clamp injury, avoids hypoperfusion of vital organs through the false lumen |
|
2. |
Yasuura K et al, 199961 |
Distal aortic arch aneurysm. n=3 Stanford type B: n=2 Replacement of descending thoractic aorta LSA reconstruction: n=1 |
Lowest temperature: 18°C Median CPB time: 175 minutes (152-215 minutes), median retrograde perfusion: 30 (29-37 minutes), median IVC flow rate: 670 (390-790 ml/min), SVC pressure: 15-18mmHg |
Nil |
Nil |
Axillary artery cannulation◻ does not require occlusion-DTA for cerebral perfusion |
BUN-blood urea nitrogen, CPB-cardiopulmonary bypass, DTA-descending thoracic aorta, IVC-inferior vena cava, LFT-liver function test, RCP-retrograde cerebral perfusion, SVC-superior vena cava
Table 5: Summary of the published clinical investigations documenting the mortality and morbidity following combined retrograde and antegrade cerebral perfusion under moderately hypothermic circulatory arrest
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables, mortality, morbidity and statistical significance |
Conclusions |
|
1. |
Kanda H et al, 2019168 |
N=23 |
Scheduled aortic arch / hemiarch, age (years) 70.4±7.44, intraoperative monitoring ocular perfusion- laser speckle flowgraphy, moderate HCA (26-28°C) in all patients for total arch and hemiarch replacements respectively. RCP 100-300 ml/min - keeping venous perfusion pressure 20 mmHg. After inspecting transverse arch SCP on all 3 vessels (BCA, LCCA, LSA), 10ml/kg/min maintain cerebral arterial pressure 45 mmHg Results: Both mean blur ratios of simple circulatory arrest and RCP significantly decreased, no significant difference between simple circulatory arrest and RCP. The mean blur ratio or SCP significantly increased compared to circulatory arrest and RCP |
Cerebral microcirculation may not be adequate during RCP compared with SCP under moderate hypothermia |
BCA-brachiocephalic artery, HCA-hypothermic circulatory arrest, LCCA-left common carotid artery, LSA-left subclavian artery, RCP-retrograde cerebral perfusion, SCP-selective antegrade cerebral perfusion
Table 6: Summary of the published clinical investigations documenting the mortality and morbidity following deep hypothermic circulatory arrest with retrograde cerebral and antegrade distal aortic perfusion
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables, mortality, morbidity, statistical significance and conclusion |
|
1. |
Bavaria JE et al, 199533 |
Study period: 1987-1994 Retrograde study of 156 patients. Elective + emergent operation of the thoracic aorta Proximal aortic surgery, n=75 Ascending aortic aneurysm, n=22 Type A dissection, n=45 Arch reconstruction, n=8 Thoracoabdominal Crawford type I, n=26 Crawford type II, n=18 Crawford type III, n=8 Crawford type IV, n=8 Traumatic transection, n=11 Type B dissection, n=10 Lowerst temperature 16° |
Proximal aortic procedure- stroke rate was 12% using CPB and 48% using HCA, additional RCP decreased stroke rate 0% (p<0.01), mortality rate 7.1% compared with 37% for HCA (p<0.005) Thoracoabdominal procedure- Straight clamping, spinal cord injury 27%, renal failure 24%, additional of distal aortic bypass- decreased spinal injury 7% (p<0.01), renal failure to 13%, distal aortic bypass decreased mortality rate 22% to 7% (p<0.05), RCP decreases the stroke rate and mortality in proximal aortic operation, distal aortic perfusion decreases the neurologic injury, renal failure and mortality in thoracoabdominal operation |
HCA-hypothermic circulatory arrest, RCP-retrograde cerebral perfusion
Table 7: Summary of the published clinical investigations documenting the mortality and morbidity following combined continuous antegrade cerebral and retrograde inferior vena caval perfusion under moderate hypothermia
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables |
Mortality |
Morbidity |
Conclusions |
|
1. |
Lin J et al, 201939 |
6 |
Study period: October 2017-November 2017 Age: 46±11 years Lowest nasopharyngeal temperature: 28-29°C Antegrade cerebral flow: 6-12 ml/kg/min rSO2±10% baseline Retrograde IVC flow: 8-12 ml/kg/min, pump pressure 20-30mmHg Two pumps are used to allow precise control of blood separately to the brain and lower body |
All survived |
Postoperative liver and renal function tests were normal |
Moderate hypothermia can reduce the duration of CPB and perturbation of coagulative function. Antegrade CBF lowers the risk of PND and retrograde perfusion provides adequate oxygenation to the key organs |
CPB-cardiopulmonary bypass, RSO2-cerebral arterial oxygen saturation, CBF-cerebral blood flow
A large retrospective German Registry for Acute Aortic Dissection Type A (GERAAADA) database study by Kruger and associates analysed 1558 patients undergoing surgery for acute type A aortic dissection in 44 cardiac surgical centres in Germany [no cerebral protection (NCP, n=88; DHCA alone, n=355, 22.8%; DHCA+RCP, n=34, 22%; DHCA+unilateral ACP, n=628, 40.3% and DHCA+bilateral ACP, n=453, 29.1%). The 30-day mortality for each cohort were 11.4%, 19.4%, unreported, 13.9% and 15.9% respectively. PND rates were 9.1%, 11.5%, unreported after correcting for mortality 10% and 11% respectively (Table 1) [13].
In order to assess the publication bias within the meta-analysis,patients with an operative mortality of 13% and PND in 3 patients [123]. In 1992, Kazui and associates used 4-branched graft technique for arch reconstruction on 32 patients with three hospital deaths and no neurological sequelae [124].
Results
The overall operative mortality and risk of cerebrovascular accidents for patients undergoing surgeries of the aortic arch using DHCA with and without antegrade or retrograde cerebral perfusion is 6% to 23% and 2% to 12% respectively among various centres practicing surgeries of the aortic arch. These patients died of diverse causes, including low cardiac output syndrome, cerebrovascular accidents, bleeding diathesis, renal failure requiring dialysis, pulmonary infection, hepatic failure and coagulopathy (Tables 1-7) [13,64-74].
Table 1: Summary of the published clinical investigations documenting the mortality and morbidity following deep hypothermic circulatory arrest and retrograde cerebral perfusion or deep hypothermic circulatory arrest and antegrade cerebral perfusion
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables |
Mortality |
Morbidity |
Conclusions |
|
1. |
Ueda Y et al, 1994 [88] |
DHCA+RCP, n=33 |
Replacement of the ascending aorta or aortic arch, intermittent and continuous RCP to extend the safe duration of HCA during arch surgeries |
In-hospital 30 days (6%) |
Stroke 6% |
RCP is a useful adjunct to DHCA upto 80 minutes to perfusion |
|
2. |
Raskin SA, 1995 [91] |
DHCA+RCP, n=88 |
Replacement of the ascending aorta or aortic arch Mean age: 63 years (range 28-78 years) Mean circulatory arrest time: 31 minutes (range 10-62 minutes) Lowest nasopharyngeal temperature: 14°C Cerebral flow-pressure: 25mmHg (upper limit) |
In-hospital 2 (2%) |
Stroke No postoperative strokes |
RCP during DHCA decreased the surgical and neurological morbidity, and has the potential for reduction of embolization of air and atheromatous debris |
|
3. |
Usui A et al, 1996 [43] |
DHCA+RCP, n=228 |
Replacement of the ascending aorta or aortic arch |
In-hospital 6.1% 30 days 13.6% |
Neurologic dysfunction: 20% |
Perfusion pressure >25 mmHg – increased incidence of cerebral edema and intracerebral bleeding |
|
4. |
Okita Y et al, 1998 [36] |
DHCA+RCP, n=50 DHCA+SACP, n=253 DHCA, n=50 CPB, n=297 |
Replacement of the ascending aorta or aortic arch |
In-hospital 6% 19% 12% 13.8% |
Cerebral complications 4% 18% 8% 3.7% |
Method cerebral perfusion did not influence outcome |
|
5. |
Bavaria JE et al, 1995 [33] |
DHCA+RCP, n=19 DHCA, n=20 CPB, n=21 |
Replacement of the ascending aorta or aortic arch |
60 day 5% 40% 19% |
CT/MRI- confirmed CVA 0% 33% 20% |
RCP resulted in less mortality than HCA. RCP resulted in fewer strokes than HCA and CPB |
|
6. |
Coselli JS and LeMaire SA, 1997 [30] |
DHCA+RCP, n-290 DHCA, n-189 |
Replacement of the ascending aorta or aortic arch |
In-hospital 30 day 3.4% 2.4% 16.9% 14.8% |
Stroke 2.4% 6.5% |
RCP resulted in less mortality and fewer strokes than HCA |
|
7. |
Coselli JS, 1997 [31] |
DHCA+RCP, n=305 DHCA, n=204 |
Replacement of the ascending aorta or aortic arch |
In-hospital 3.9% 17.16% |
Stroke 2.62% 6.37% |
RCP resulted in less mortality and fewer strokes than HCA |
|
8. |
Safi H et al, 1997 [25] |
DHCA+RCP, n=120 HCA, n=41 |
Replacement of the ascending aorta or aortic arch |
Nil |
CT/MRI-confirmed stroke 2.5% 9.8% |
RCP resulted in significantly fewer strokes than HCA |
|
9. |
Moshkovitz Y et al, 1998-95 |
Moderate HCA+RCP at 10°C, n=104 |
Replacement of the ascending aorta or aortic arch, moderate HCA (22-26°C, RCP at 10°C) |
In-hospital 7.7% |
Stroke 7.7% Seizures 3.8% |
Combination of moderate HCA with RCP at 10°C- safe upto 30 minutes of HCA |
|
10. |
Ehrlich M et al, 1998 [41] |
DHCA+RCP, n=28 DHCA, n=65 |
Replacement of the ascending aorta or aortic arch |
30 day 14% 40$ |
Neurological dysfunction 10% 21% |
RCP resulted in less mortality and neurological dysfunction than HCA |
|
11. |
Usui A et al, 2012 [162] |
DHCA+RCP, n=75 SACP, n=91 |
Replacement of the ascending aorta or aortic arch |
In-hospital 24% 21% |
Neurologic dysfunction 16% 19% |
No difference between RCP and SCP in death or neurologic dysfunction |
|
12 |
Okita Y et al, 2001 [37] |
DHCA+RCP, n=76 DHCA+SACP, n=112 Partial CPB, n=58 |
Replacement of the ascending aorta or aortic arch |
In-hospital Late 8% 4% 23% 3% 21% 28% |
Stroke 4% 11% 24% |
Method of cerebral perfusion did not influence outcome |
|
13. |
Moon MR et al, 2002 [139] |
DHCA alone, n=36 DHCA+RCP, n=36 |
Study period 1996-2000 Lowest core temperature — 18°C±2°C (12-24°C) DHCA: 19.5±2.3 DHCA+RCP: 19.2±3.2 p=0.64 |
In-hospital 8.1±5% 11±5% p>0.95 |
Neurological deficits 14%±6% 14%±6% p>0.73 |
Supplmental RCP during HCA did not decrease mortality or neurologic complications. Retrograde rewarming through femoral artery increased transient neurological dysfunction. RCP remains optional. Reperfusion should be antegrade |
|
14. |
Yamashita C et al, 1998 [35] |
38 patients |
Study period: 1986-1996 Distal aortic arch aneurysm, Group I- graft anastomosis with ACC and left heart bypass (1986-89), MS+ALT= 9, PLT=7 Group II: MS+ALT, open anastomosis, graft anastomosis, RCP, DHCA Group III- open anastomosis with RCP in Trendelenburg position, PLT |
Hospital death Group I: 25% (4/16), died of stroke, MI Group II: 37.5% (3/8), respiratory failure, aortic dissection Group III: 7.1% (1/14), congestive cardiac failure |
Nil |
RCP with a posterolateral thoracotomy minimizes the risk of stroke and respiratory failure during arch operation |
|
15. |
Tonoue Y et al, 1999 [28] |
RCP, n=15 ACP, n=17 |
Study period: 1993-1997 Lowest nasopharyngeal temperature: 15.9°C Perfusion time (min): RCP (38.3±1.46); ACP (71.9±40.4) Pump flow rate (ml/min): RCP (459±270); ACP (500) Perfusion pressure (mmHg): RCP (22.7±4.0); ACP (35.1±12.5) Tympanic membrane (°C): RCP (16.7±2.2); ACP (15.9±3.5) |
RCP, n=2 (stroke) SCP, n=1 (bleeding) |
SCP stroke, n=3 |
The measurement on middle cerebral artery blood flow velocities with transcranial doppler is practicable during SC, difficult during RCP indicating critical decrease in CBF during RCP |
|
16. |
Coselli JS, 1994 [32] |
DHCA+RCP, n=88 |
Study period: 1992-93 Arch repair – DHCA circulatory arrest CPB time-113 (range 66-216 minutes), circulatory arrest 31 (10-62 minutes), EEG- isoelectric at nasopharyngeal temperature 72°C to 25.4°C |
30 days mortality, n=2 |
No postoperative stroke |
Clinically safe method ◻ DHCA+RCP |
|
17. |
Okamoto H et al, 1993 [54] |
RCP (conventional), n=19 RCP (selective), n=34 |
Aortic arch operation |
RCP (conventional), n=1 RCP (selective)- no event including 2 patients with RCP >100 minutes |
Nil |
10-20% patients have functioning venous valves at jugular-subclavian junction which may interfere with RCP. Satisfactory cerebral protection should be possible with selective RCP >60 min |
|
18. |
Bonser RS et al, 1999 [39] |
DHCA. n=21 DHCA+RCP, n=21 |
Lowest NP temperature: 15°C SVC perfusion: 25 mmHg, transcranial paired arterial and jugular bulb blood: oxygen, glucose HCA duration min (mean±SD): HCA (32±9); RCP (27±12.3); p=0.14 RCP duration min (mean±SD): (23±9.6) CPB duration min (mean±SD): HCA (145±24.3); RCP (153±35.7), p=0.4 Ascending aortic + aortic root resection: HCA (n=13), RCP (n=13) Hemiarch± root: HCA (n=3), RCP (n=3) Total arch± root: HCA (n=3), RCP (n=3) |
Hospital death DHCA, n=1 RCP, n=2 Permanent neurological deficit DHCA, n=1 RCP, n=0 Transient neurological deficit DHCA, n=0 RCP, n=2 |
Nil |
Transcranial oxygen extraction during RCP 3.3 ml/dl, range 0.7- 6.6 ml/dl, significantly higher than extraction with antegrade perfusion before and after HCA (p<0.1), RCP flow was insufficient to maintain cerebral oxygenation, RCP may improve cerebral protection through other mechanism |
|
19. |
Lau C et al, 2018 [134] |
1043 patients |
Study period: 1997-2014 Age mean: 65.7±13.3 years, DHCA + RCP perfusion time >50 minutes <49 minutes P value Number 50 993 Age (years) 61.2±13.4 65.9±13.3 0.014 |
Mortality group >50 min versus 49 min, 8% vs 3.8% (p=0.14), stroke rate 2% vs 1.2% (p=0.62), propensity matching resulted in 48 pairs. DHCA duration was not independently associated with operative death or postoperative neuro deficits. RCP- effective adjunctive cerebral protection strategy for aortic arch aneurysm surgeries, not associated with increased death or neurological complications |
||
|
20. |
Wong CH and Bosner RS, 1999 [45] |
DHCA, n=34 DHCA+RCP, n=96 |
Study period 1991-1998 Age: 2-=84 years (mean 62.7 years) Emergent surgery 46/130 (35.4%), lowest temperature 15°C, alpha stat pH DHCA- arrest duration 30.1 min (2-80 minutes) , p<0.019 DHCA+ RCP- circulatory arrest 24.4 (8-53 minutes), p<0.019 Multivariate logistic regression- RCP duration (p<0.038) as risk factors for mortality, and myocardial ischemic time (0.012) ahd HCA duration (p=0.05) as risk factor for stroke. HCA and RCP groups differed in HCA duration (HCA mean 25 min (10-80), RCP mean 32 min (10-69), p<0.019 Mortality: DHCA+RCP (15%), Stroke (7%) DHCA alone (24%), Stroke (6%) |
Age and HCA remain risk factors for stroke and mortality despite RCP, HCA times were longer in the RCP patients, patients were not randomized |
||
|
21. |
Esmailian F et al, 1999 [32] |
52 patients |
Study period: 1991-1998 Age 3 weeks-89 years, mean RCP time 39.5 minutes (3-88 minutes), RCP >45 min, n=16 (31%) Core temperature 19.3 (15-27°C), RCP >45 min, n=12 - no. CVA, RCP >70 min, n=2- major CVA-died, subdural hematoma, n=1 Temporary mental abnormality, normal CT |
RCP-reliable and technically appealing, removed air, particulate matter |
||
|
22. |
Ganapati AM et al, 2014 [71] |
DHCA+ACP, n=360 DHCA+RCP. N=80 Propensity matched ACP, n=40 RCP, n=40 |
Study period: 2005-2013 Propensity matched analysis – DHCA+ACP vs DHCA + RCP – hemi arch replacement, a propensity score with 1:1 matching of 40 pre and intraoperative variables used to adjust for differences between groups Between ACP and RCP- no differences in 30 day/in-hospital mortality or morbidity outcomes, total arch cases were excluded to limit the analysis to shorter DHCA times and a more uniform patient population |
In proximal arch operations using DHCA, equivalent early and late outcomes can be achieved with RCP and AC |
||
|
23. |
Hu Z et al, 2014 [70] |
DHCA+ACP, n=2855 DHCA+RCP, n=1897 |
15 studies; pooled analysis- no difference in 30 day mortality, PND & PND in the 2 groups |
ACP and RCP provide similar protective effectiveness combined with DHCA and could be selected according to the actual condition in aortic arch surgery |
||
|
24. |
Guo S et al, 2015 [66] |
DHCA+ACP, n=4262 DHCA+RCP, n=2761 |
Meta-analysis of 34 studies TND-risk ratio 0.72 (95% CI 0.58-0.90); Z score 2.9, p=0.004 Patients undergoing DHCA+ACP- better outcomes in terms of TND compared to DHCA+RCP No difference between group in terms of PND, stroke and early mortality |
DHCA+ACP has an advantage over DHCA+RCP in terms of TND, while the two methods show similar results in terms of PND, early mortality and stroke |
||
|
25. |
Okita Y et al, 2015 [115] |
ACP, n=7038 HCA+RCP, n=114 |
Study period: 2009-2012 Total arch replacements, n=16218 ACP vs HCA+RCP, analysis on 8169 patients (ascending aortic dissection, ruptured aneurysm, emergency surgery – excluded) 30 day mortality 3.2% vs 4.0%, hospital death 6.0% vs 7.1%, stroke 6.7% vs 8.6%, TND 4.1% vs 4.4%, no difference in composite outcome of hospital death, stroke, need for dialysis, prolonged ICU stay > 8 days 24.2% vs 15.6% with HCA/RCP |
Both techniques provide comparable clinical outcomes with regard to mortality, stroke rate. HCA/RCP – prolonged ICU stay |
||
|
26. |
Tian DH et al, 2018 [65] |
HCA, n=2705 HCA+RCP, n=2817 |
Twenty-eight comparative studies that included patient groups undergoing aortic arch surgery using HCA or HCA+RCP Significantly increased mortality – DHCA compared to DHCA + RCP, odds ratio 1.75, 95% CI: 1.16-2.63, p=0.007, I2 54%; stroke significant increase in HCA group (OR 1.5, 95% CI: 1.07-2.90, p=0.02), I2 29%; temporary neurodeficits- no difference (p=0.66) |
Addition of RCP may provide better outcomes than using HCA alone |
||
|
27. |
Hameed I et al, 2019 [74] |
ACP, n=15293 RCP, n=7511 DHCA, n=4164 |
68 studies, n=26968 patients; USA, n=19; Japan, n=13; Germany, n=6; other countries, n=30 6 randomized controlled trials (n=354), 62 observational studies (n=26,614), Mean age: ACP 48.1-71 years, RCP 48.5-71 years, DHCA 49-68.1 years; compared with DHCA, both ACP and RCP were associated with significantly lower postoperative stroke and operative mortality rates, ACP odds ratio 0.62 (95% CI: 0.51-0.75) odds ratio 0.66 (95% CI: 0.51- 0.76) respectively RCP odds ratio 0.66 (95% CI: 0.54-0.82), odds ratio 0.57 (95% CI: 0.45-0.71) respectively; ACP and RCP associated with similar incidence of primary outcome; relative benefit increases with the duration of circulatory arrest. |
No difference among 3 techniques on secondary outcome. Unilateral or bilateral antegrade cerebral perfusion did not influence the results, when arrest time exceeded 25 min- the benefits of RCP, ACP over DHCA become significant |
||
|
28. |
Ganzel, BL et al 1997 [132] |
Study period: 1993-1996 Complex aortic and aortic arch surgeries- neurophysiologic monitoring DHCA+RCP, n=22 DHCA alone, n=8 Circulatory arrest duration (min) 26 (22-30) 24 (15-33) Temperature °C 17 (16-19) 17 (14-20) Decrease of regional cerebral venous oxygen saturation |
Under the guidance of multimodality neurologic monitoring, high flow RCP as safe as circulatory arrest alone |
|||
|
29. |
Tian DH et al, 2013 [64] |
Aortic arch operation, meta-analysis of 9 studies, DHCA alone n=64.8, DHCA+SACP n=370; DHCA+SACP was associated with superior survival outcomes (p=0.008), i2=0%. No difference in permanent neurologic outcomes |
DHCA+SACP was superior to DHCA alone |
|||
|
30. |
Okita Y et al, 2001 [37] |
Study period: 1997-1999, total aortic arch replacement; DHCA+RCP, n=30; DHCA+SACP=30 Hospital death: RCP (6.6%; SCP (6.6%) New strokes: RCP (3.3%), SCP (6.6%), p=0.6 TND: RCP (33.3%), SCP 13.(3%), p=0.05 |
Both methods of cerebral protection resulted in acceptable morbidity and mortality. The prevalence of TND was significant higher in RCP |
|||
|
31. |
Gatti G et al, 2017 [150] |
Study period: 1999-2015; aortic arch operation DHCA 14-20°; DHCA+RCP=344, DHCA alone= 26 (control group), in hospital death (9.6%), PND (9%), TND (19.1%) |
DHCA+RCP- low risk of TND provided DHCA <25 min |
|||
Table 2: Summary of the published clinical investigations documenting the mortality and morbidity following deep hypothermic circulatory arrest + retrograde cerebral perfusion, moderately hypothermic circulatory arrest and antegrade cerebral perfusion
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables, mortality, morbidity and statistical significance |
Conclusions |
|
1. |
Milewski RK et al, 2010154 |
DHCA+RCP, n=682 MHCA+ACP, n=94 |
Study period: 1997-2008 Analysis of two institutions; mean cerebral ischemic time and visceral ischemic time differed between RCP/DHCA and ACP/MHCA (p<0.001). There was no significant difference in permanent neurologic, deficit, temporary neurologic dysfunction, or renal failure, between RCP/DHCA and ACP/MHCA on multivariate analysis. Mortality was comparable across both techniques |
Both techniques have emerged as effective techniques for selected aortic arch operations with low morbidity and mortality, no statistically significant difference in primary or secondary outcomes between techniques for aortic reconstruction times less than 45 minutes |
|
Study period: 2006-2014 |
MHCA/ACP was associated with 76.5% decreased risk (RR 0.23, 95% CI: 0.07 to 0.69) of postoperative neurologic complications (p=0.009), mid-term all cause mortality MHCA/ ACP modestly decreased the number of deaths (p=0.04), MHCA/ACP- a trend towards decreased 30 day and mid-term mortality |
|||
|
Propensity score matching analysis of 259 patients, after propensity scoring 40 pairs (80 patients) matched |
||||
|
Before matching |
||||
|
2. |
Perreas K et al, 2016163 |
Ascending aortic + hemiarch correction, n=259 DHCA/RCP, n=207 |
After matching |
|
|
MHCA/ACP. n=52 |
DHCA/ RCP |
|||
|
MHCA/ ACP |
||||
|
P value |
||||
|
DHCA/ RCP |
||||
|
MHCA/ ACP |
||||
|
P value |
||||
|
3. |
Leshnower BG et al, 2019102 |
DHCA+RCP, n=11 MHCA+ACP, n=9 |
Hemiarch replacement, nasopharyngeal temperature Stroke p value DHCA+RCP 19.9°±0.1°C (p<0.0001) 5/11 (45%) 0.01 MHCA+ACP 26.3°±1.8°C 9/9 (100%) Mortality / renal failure – Nil |
MHCA + ACP may be associated with a higher incidence of radiographic neurologic injury than DHCA + RCP in patients undergoing hemiarch replacement |
ACP-antegrade cerebral perfusion, CI-confidence interval, DHCA-deep hypothermic circulatory arrest, MHCA-moderate hypothermic circulatory arrest, RCP-retrograde cerebral perfusion,
Table 3: Summary of the published clinical investigations documenting the mortality and morbidity following deep hypothermic circulatory arrest and intermittent pressure augmented retrograde cerebral perfusion
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables, mortality, morbidity and statistical significance |
Conclusions |
|
1. |
Kubota H et al, 201053 |
25 years female |
Diagnosis aortitis with ascending aortic arch aneurysm, CT-aneurysm from ascending aorta to aortic arch, maximum diameter 76 mm, MR angio- occlusion- BCA, LSA, right brain perfused via LICA, Echo-severe AR, bioprosthetic AVR: 21mm, total ascending aortic and arch replacement, reimplantation- BCA, LCCA, lowest temperature: 18°C, circulatory arrest, IPA-RCP, SVC pressure 15-20 mmHg x 2 min, 45 mmHg x 30 seconds, repeated every 20 minutes, duration- IPA-RCP: 75 minutes, RSO2 maintained: 80-85%, postoperative brain perfusion scintigraphy-improved perfusion- right cerebral hemisphere |
IPA-RCP may contribute to brain protection and better clinical outcomes |
|
2. |
Endo H et al, 201352 |
DHCA-CRCP, n=10 DHCA-IPA-RCP, n=10 |
Study period: 2005-2008 DHCA-CRCP – continuous venous pressure 25mmHg DHCA-IPA-RCP – venous pressure 20mmHg (120 seconds), 45 mmHg (30 seconds) rSO2- near infraread spectroscopy every 10 min Mortality- Nil, major neurological complications – nil Full wakefulness – end of surgery to fully awake- conventional RCP 310±282 min, IPA-RCP 85±64 min (p<0.5) rSO2 greater than conventional RCP from 10-70 mmHg (p<0.5) |
IPA-RCP provides more homogenous cerebral perfusion and a more effective supply |
AR-aortic regurgitation, AVR-aortic valve replacement, BCA-brachiocephalic artery, CT-computed tomography, IPA-RCP- intermittent pressure augmented retrograde cerebral perfusion, LCCA-left common carotid artery, LICA-left internal carotid artery, LSA-left subclavian artery, RSO2-cerebral arterial oxygen saturation, SVC superior vena cava
Table 4: Summary of the published clinical investigations documenting the mortality and morbidity following deep hypothermic circulatory arrest and retrograde coronary sinus and retrograde superior and inferior vena caval perfusion
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables |
Mortality |
Morbidity |
Conclusions |
|
1. |
Yasuura K et al, 199259 |
5 patients |
Study period: 1990-1991 Age: 18-59 years, Median: 54 years, ascending aortic replacement±Bentall, CPB mean time: 253 (range 162-351 minutes), rectal temperature during RCP: 16-20°C, mean time total RCP: 82 minutes (range 32-110 minutes) |
Nil |
No neurological complications, postoperative BUN: 28-30 mg/dl, serum creatining 1.5-1.8 mg/ dl, LFT-normal |
Total body retrograde perfusion creates a relatively bloodless field, permits complete repair without fear of clamp injury, avoids hypoperfusion of vital organs through the false lumen |
|
2. |
Yasuura K et al, 199961 |
Distal aortic arch aneurysm. n=3 Stanford type B: n=2 Replacement of descending thoractic aorta LSA reconstruction: n=1 |
Lowest temperature: 18°C Median CPB time: 175 minutes (152-215 minutes), median retrograde perfusion: 30 (29-37 minutes), median IVC flow rate: 670 (390-790 ml/min), SVC pressure: 15-18mmHg |
Nil |
Nil |
Axillary artery cannulation◻ does not require occlusion-DTA for cerebral perfusion |
BUN-blood urea nitrogen, CPB-cardiopulmonary bypass, DTA-descending thoracic aorta, IVC-inferior vena cava, LFT-liver function test, RCP-retrograde cerebral perfusion, SVC-superior vena cava
Table 5: Summary of the published clinical investigations documenting the mortality and morbidity following combined retrograde and antegrade cerebral perfusion under moderately hypothermic circulatory arrest
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables, mortality, morbidity and statistical significance |
Conclusions |
|
1. |
Kanda H et al, 2019168 |
N=23 |
Scheduled aortic arch / hemiarch, age (years) 70.4±7.44, intraoperative monitoring ocular perfusion- laser speckle flowgraphy, moderate HCA (26-28°C) in all patients for total arch and hemiarch replacements respectively. RCP 100-300 ml/min - keeping venous perfusion pressure 20 mmHg. After inspecting transverse arch SCP on all 3 vessels (BCA, LCCA, LSA), 10ml/kg/min maintain cerebral arterial pressure 45 mmHg Results: Both mean blur ratios of simple circulatory arrest and RCP significantly decreased, no significant difference between simple circulatory arrest and RCP. The mean blur ratio or SCP significantly increased compared to circulatory arrest and RCP |
Cerebral microcirculation may not be adequate during RCP compared with SCP under moderate hypothermia |
BCA-brachiocephalic artery, HCA-hypothermic circulatory arrest, LCCA-left common carotid artery, LSA-left subclavian artery, RCP-retrograde cerebral perfusion, SCP-selective antegrade cerebral perfusion
Table 6: Summary of the published clinical investigations documenting the mortality and morbidity following deep hypothermic circulatory arrest with retrograde cerebral and antegrade distal aortic perfusion
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables, mortality, morbidity, statistical significance and conclusion |
|
1. |
Bavaria JE et al, 199533 |
Study period: 1987-1994 Retrograde study of 156 patients. Elective + emergent operation of the thoracic aorta Proximal aortic surgery, n=75 Ascending aortic aneurysm, n=22 Type A dissection, n=45 Arch reconstruction, n=8 Thoracoabdominal Crawford type I, n=26 Crawford type II, n=18 Crawford type III, n=8 Crawford type IV, n=8 Traumatic transection, n=11 Type B dissection, n=10 Lowerst temperature 16° |
Proximal aortic procedure- stroke rate was 12% using CPB and 48% using HCA, additional RCP decreased stroke rate 0% (p<0.01), mortality rate 7.1% compared with 37% for HCA (p<0.005) Thoracoabdominal procedure- Straight clamping, spinal cord injury 27%, renal failure 24%, additional of distal aortic bypass- decreased spinal injury 7% (p<0.01), renal failure to 13%, distal aortic bypass decreased mortality rate 22% to 7% (p<0.05), RCP decreases the stroke rate and mortality in proximal aortic operation, distal aortic perfusion decreases the neurologic injury, renal failure and mortality in thoracoabdominal operation |
HCA-hypothermic circulatory arrest, RCP-retrograde cerebral perfusion
Table 7: Summary of the published clinical investigations documenting the mortality and morbidity following combined continuous antegrade cerebral and retrograde inferior vena caval perfusion under moderate hypothermia
|
S. No. |
Authors |
No. of patients |
Patient demographics and operative variables |
Mortality |
Morbidity |
Conclusions |
|
1. |
Lin J et al, 201939 |
6 |
Study period: October 2017-November 2017 Age: 46±11 years Lowest nasopharyngeal temperature: 28-29°C Antegrade cerebral flow: 6-12 ml/kg/min rSO2±10% baseline Retrograde IVC flow: 8-12 ml/kg/min, pump pressure 20-30mmHg Two pumps are used to allow precise control of blood separately to the brain and lower body |
All survived |
Postoperative liver and renal function tests were normal |
Moderate hypothermia can reduce the duration of CPB and perturbation of coagulative function. Antegrade CBF lowers the risk of PND and retrograde perfusion provides adequate oxygenation to the key organs |
CPB-cardiopulmonary bypass, RSO2-cerebral arterial oxygen saturation, CBF-cerebral blood flow
A large retrospective German Registry for Acute Aortic Dissection Type A (GERAAADA) database study by Kruger and associates analysed 1558 patients undergoing surgery for acute type A aortic dissection in 44 cardiac surgical centres in Germany [no cerebral protection (NCP, n=88; DHCA alone, n=355, 22.8%; DHCA+RCP, n=34, 22%; DHCA+unilateral ACP, n=628, 40.3% and DHCA+bilateral ACP, n=453, 29.1%). The 30-day mortality for each cohort were 11.4%, 19.4%, unreported, 13.9% and 15.9% respectively. PND rates were 9.1%, 11.5%, unreported after correcting for mortality 10% and 11% respectively (Table 1) [13].
In order to assess the publication bias within the meta-analysis,patients with an operative mortality of 13% and PND in 3 patients [123]. In 1992, Kazui and associates used 4-branched graft technique for arch reconstruction on 32 patients with three hospital deaths and no neurological sequelae [124].
Discussion
Since the introduction of DHCA for surgeries of aortic arch, controversy persists regarding the optimal strategy for cerebral protection during planned and emergent aortic surgeries. Five different options of cerebral protection currently exist: DHCA alone, unilateral or bilateral antegrade cerebral perfusion, retrograde cerebral perfusion with moderate or deep hypothermic circulatory arrest, and total body retrograde perfusion. Each strategy has its own risks and benefits, but the surgical community has endorsed no single strategy.
Although there have been major advances in the methods of cerebral protection, since the inception of open heart surgery, surgeries on the transverse aortic arch have never the less remained far from unhurried because of the anaerobic damage that can occur with all current methods of cerebral protection. The ideal cerebral protection strategies should provide excellent preservation with minimal organic cerebral damage and mortality. The efficacy of cerebral protection is gauged by safe periods of cerebral ischemic time that it affords the surgeon.
Deep hypothermic circulatory arrest alone
Initially, aortic arch operations with DHCA without an adjunct were critically limited to short duration of 30 minutes (less than 40 minutes in more contemporary series) [75-79,125,126]. If prolonged beyond 50 minutes, it resulted in cerebral stroke rates up to 16.7% and marked increase in mortality rate after 65 minutes [126-137]. Transient neurologic dysfunction (TND) is defined as confusion, agitation, delirium, prolonged obtundation or Parkinsonism in the immediate postoperative period is also common, occurring in 14% to 37% of patients (Table 1) [135-143].
A 2013 consensus statement by Yan et al defined 4 categories of HCA: profound (<14°C), deep (14.1°C -20.0°C), moderate (20.1°C -28.0°C), and mild (28.1°C -34.0°C). The statement suggested a safe HCA duration of 30-to-40 minutes at profound HCA, 20-to-30 minutes at deep HCA, 10-to-20 minutes at moderate, fewer than 10 minutes at mild HCA. The statement further suggested that axillary artery cannulation allows for the later institution of ACP to provide perfusion during HCA [144].
Deep hypothermic circulatory arrest with adjunct retrograde cerebral perfusion
Between 1996 and 2002, a number of clinical reports have suggested that retrograde cerebral perfusion as an adjunct to DHCA can dramatically improve the operative outcome of aortic arch surgeries [25-33,41,42,45-47,72,90]. Most of these studies, however, have compared contemporary results with historic controls. The improvements in surgical results during the past two decades are multifactorial considering the advancements in neurologic monitoring, and surgical techniques, making comparisons to historic controls imprudent.
It has been shown in experimental animals, using tracking of fluorescent microspheres, magnetic resonance perfusion scans and intra vital microscopy, [146,147] that only 0.01% of perfusate flow transits through the brain parenchyma itself, with the majority being sequestered or bypassed through non-brain capillaries [148]. Despite this, canine and porcine models have also revealed that although not ideal, RCP does indeed provide superior metabolic support compared with HCA alone, as measured through lactate and adenosine triphosphate elimination with similar superior outcomes also seen in histologic and animal studies [25-28,129-131,149].
The primary concern for RCP has been the risk of cerebral edema due to hyper perfusion. As RCP pressure increases, a corresponding increase in cerebral edema has been identified in animals [130,131,149]. Clinically, however, Ganzel and colleagues have shown that with extensive intraoperative neurophysiologic monitoring, RCP flow can be safely titrated and cerebral edema avoided [132].
Two investigators (Deeb and colleagues, Ganzel and colleagues) demonstrated the results of RCP, with a mean RCP pressure of 40mmHg (30-49 mmHg) and flow rate of 1.2 L/min with a <10% incidence of neuro deficit. The mean RCP time was 63 minutes (range 35 to 128 minutes) [132,151]. Ueda and associates first reported that RCP is a useful adjunct to DHCA in augmenting cerebral protection for up to 80 minutes [152]. Coselli and LeMaire reported lower mortality (7.9% vs 14.8%) and stroke rates (2.4% vs 6.5) among 479 patients undergoing surgeries of the aortic arch under DHCA with and without RCP respectively [30]. Safi and associates demonstrated that RCP had a protective effect against stroke (3% vs 9%) [26]. Bavaria and associates reported that for DHCA exceeding 60 min, RCP improved mortality and morbidity [135]. However, an increased incidence of TND has been demonstrated with the duration of RCP exceeding 25 minutes [153]. These excellent results were in stark contrast with earlier dismal experience with arrest-only periods exceeding 60 minutes (Table 1) [154].
There are several explanations for the superior results of adjunct RCP compared to isolated DHCA. First, animal studies using microspheres have confirmed the ability for RCP to flush particulate and gaseous emboli from the arterial tree, thereby reducing embolic load and the risk of stroke [130,131,133]. Second, RCP offers more consistent and continuous cerebral cooling. Finally, although RCP is not able to adequately fulfil cerebral metabolic demand, its limited flow can aid in removing neurotoxic metabolites [130,131,133].
Deep hypothermic circulatory arrest with adjunct antegrade cerebral perfusion
The routine use of RCP has decreased significantly over the past three decades supplanted by the growing acceptance of ACP [127,128]. Antegrade cerebral perfusion has shown to be superior to RCP in providing physiologically relevant cerebral blood flow with respect to cerebral metabolism and preserving the cellular structure on histopathology analysis [141]. DiEusanio and associates demonstrated that ACP longer than 90 minutes is not associated with an increased risk of mortality or neurological events [155]. After the report by Spilvogel and associates, an “arch first” approach using a branched graft has become a standard procedure permitting a reduction of cerebral ischemia time compared with the “distal first anastomosis” technique [156].
The criticism of ACP include longer operating time for arch reconstruction, cannulation generated embolism and uneven distribution of cerebral blood flow. Analysis of mortality and morbidity by several investigators has demonstrated that the risk factors for perioperative stroke were severity of leukoaraiosis of the brain white matter and the presence of a “shaggy” aorta. The risk factors for TND were shaggy aorta, leukoaraiosis, carotid artery lesion and duration of CPB. These investigators concluded that postoperative stroke is primarily patient and pathology dependent, and is only marginally affected by the cerebral protection strategy [157-159].
It is pertinent to state that all the quoted meta-analyses in the published literature till 2018 were pairwise comparisons. In 2019, Hameed and associates performed the first Network Meta-Analysis (NMA) comparing all 3 cerebral protection strategies, namely DHCA, DHCA+RCP and DHCA+ACP. ACP and RCP were associated with significantly lower postoperative stroke and operative mortality rates compared with DHCA. Of note, the difference in favour of both ACP and RCP compared with DHCA increased with the duration of the arrest. When the arrest time exceeds 25 minutes, the benefits of ACP and RCP over DHCA became significant. These investigators found no difference between ACP and RCP for all the explored outcomes, although at meta-regression, the use of moderate hypothermia was associated with better results in the ACP arm, and the duration of arrest was associated with better results in the RCP arm. Of note, the use of unilateral or bilateral ACP did not affect the results of the comparison with the other neuroprotective strategies [74].
The results of Hameed and associates are similar to those of Englum and associates, who compared all the different combinations of neuroprotection during aortic arch surgery using data of 12,521 patients from the STS Database and found that DHCA was associated with the highest risk of the combined end point of operative mortality or neurologic complication [73].
Most of these studies reached the same conclusion that DHCA+ACP or RCP are better than DHCA alone, especially when the requiring brain protection time is longer than 30 minutes and history of central neurologic events is a predictor of postoperative stroke [20,24,70,112,127,153,160].
Several studies have reported that PND is more likely to occur after ACP because of embolism and TND was more likely to occur after RCP because of global ischemia and a longer cerebral ischemic time. In the meta-analysis by Hu and associates, there was no difference in TND and PND between the RCP group and the ACP group, suggesting that both techniques provide acceptable cerebral outcomes. The technique best suited to the individual patient can therefore be selected [70-74].
With shorter hypothermic circulatory arrest, the differences in metabolic support provided by antegrade or retrograde cerebral perfusion are less important and are superseded by the prevention of embolic phenomena. In a prospective randomized study on 20 patients undergoing transverse hemiarch replacement receiving either DHCA+RCP (14.1-20°C) or MHCA+ACP (core temperature 20-28°C), Leshnower and associates observed no significant difference in clinically evident neurologic injury. However, a significantly higher incidence of radiographic (diffusion-weighted MRI) neurologic injury was observed with MHCA+ACP group. The reduction of silent infarcts observed in the DHCA+RCP patients in this study by Leshnower could be due to prevention of embolic phenomena [99-101]. Juvonen and associates demonstrated the same phenomena of washing out of microspheres with retrograde cerebral perfusion and inferior vena caval occlusion, experimentally in a porcine model (Table 2) [13,131].
In 2015, investigators extracted data from 8169 patients registered in Japanese Adult Cardiovascular Surgery Database undergoing total arch replacement with reconstruction of the three arch vessels from January 2009 and December 2012 and detected no significant difference between ACP and DHCA + RCP with regard to operative mortality, stroke and TND; however, there was a tendency towards a higher incidence of these indices in the RCP group [72].
In a prospective randomized neurocognitive and S-100 study of DHCA, RCP, and ACP, Svensson and associates demonstrated no difference among hypothermic circulatory arrest, antegrade cerebral perfusion and retrograde cerebral perfusion groups [83].
Retrospective analysis of 717 survivors of ascending and aortic arch surgery by Hagl and associates demonstrated that the method of brain protection did not influence the incidence of stroke and ACP did result in significant reduction in the incidence of TND [153]. In 2004, Barnard and colleagues assessed 408 studies of DHCA and ACP and reported that adjunct ACP with DHCA was superior to DHCA alone [161]. However, their clinical evidence was weak.
In a propensity matched analysis from Japanese database on data from 2792 patients undergoing aortic arch surgery with adjunct antegrade or retrograde cerebral perfusion, Usui and associates concluded that there was no difference regarding postoperative survival or neurologic outcomes except for a higher incidence of temporary dialysis and TND in the retrograde cerebral perfusion group [162].
However, the data was skewed because of the mixture of hemiarch and total arch replacement in their study. A recent meta-analysis of 5060 patients in 15 studies by Hu and associates demonstrated equal incidence of postoperative stroke and TND by antegrade and retrograde cerebral perfusion [70].
Deep hypothermic circulatory arrest with adjunct antegrade or retrograde cerebral perfusion: Which is superior?
Although literature documents equivalent neuroprotection for patients undergoing total arch replacement with antegrade or retrograde cerebral perfusion, there is a consensus among aortic surgeons that antegrade cerebral perfusion is the preferred method of cerebral perfusion for prolonged periods of circulatory arrest [35-38,75,99-101]. A recent survey shows that most European surgeons use ACP and RCP for emergency cases, whereas in US, data from 2017 STS Database show that DHCA is the most commonly used method (Tables 1,2) [73,127]. Overall pooled comparative results of meta-analyses in the published literature by Forest plot analysis demonstrated equal postoperative mortality outcome between DHCA+ACP vs DHCA+RCP. However, there was a slightly increased incidence of TND and PND among patients undergoing DHCA+ACP as compared to DHCA+RCP (Figures 1-3).
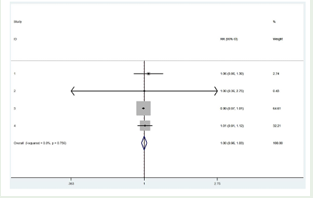
Figure 1: Forest plot of comparison of early mortality of ACP (left) versus RCP (right). RR-relative risk; CI-confidence interval; Study ID: 1 Ganapati AM et al. [71], Okita Y et al.[115], Hu Z et al. [70], Okita Y et al, [37].
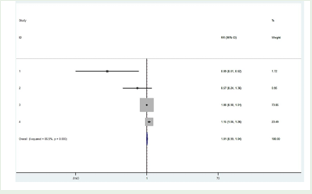
Figure 2: Forest plot of comparison of permanent neurological dysfunction of ACP (left) versus RCP (right). RR-relative risk; CI-confidence interval; Study ID: 1 Ganapati AM et al. [71], Okita Y et al. [115], Hu Z et al. [70], Okita Y et al, [37].
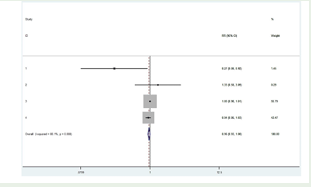
Figure 3: Forest plot of comparison of temporary neurological dysfunction of ACP (left) versus RCP (right). RR-relative risk; CI-confidence interval; Study ID: 1 Ganapati AM et al. [71], Okita Y et al. [115], Hu Z et al. [70], Okita Y et al, [37].
Moderately hypothermic circulatory arrest with adjunct antegrade cerebral perfusion
In recent years, there has been a tendency towards moderate hypothermia during aortic arch reconstruction surgeries to decrease the duration of CPB and to limit the risk of neurologic injury.163 There is uniform agreement among the proponents of the moderate hypothermic group of investigators not to go above 26°C (nasopharyngeal temperature), because higher temperatures can predispose the visceral organs and spinal cord at risk of ischemic injury [17,33,99-101,154]. However, some investigators have demonstrated that warmer body temperature is a risk factor for spinal cord ischemia during circulatory arrest [17,99-101]. At Emory, MHCA+ACP is the preferred neuro protection strategy for patients undergoing total aortic replacement with anticipated extended duration of circulatory arrest (Table 2) [99-101].
Unilateral versus bilateral selective antegrade cerebral perfusion
The majority of European centres prefer bilateral selective antegrade cerebral perfusion. However, 38% in acute condition and 33% in the chronic condition adopts unilateral antegrade perfusion [127,164,165]. During selective unilateral ACP, contralateral perfusion depends on collateral pathways, most prominently the circle of Willis. The incidence of incomplete circle of Willis varies. In autopsy study of 98 human brains, Merkkola and associates demonstrated incomplete circle of Willis in 17% of specimens [166]. In a study of 500 circles by Papantchev and associates, 42.4% of eastern European had an incomplete circle of Willis [167]. In a series of 99 arch replacements using unilateral selective ACP (30°Cx18minutes) in a left common carotid artery, Urbanski and associates noted good contralateral perfusion in all patients [168]. This study underpins the importance of collateral vessels, such as ophthalmic artery, leptomeningeal vessels and external carotid arteries. Available data indicate bilateral ACP has no significant benefits over unilateral ACP in 30-day mortality, TND or PND.
Protocol of intermittent pressure augmented-retrograde cerebral perfusion and total body retrograde perfusion
Retrograde cerebral perfusion with augmentation of CVP to 15 mmHg to 20 mmHg is commonly used for additional brain protection. However, at these pressures, the intracranial vessels do not fully open. To overcome this drawback Endo & associates and Kubota & associates successfully clinically applied the protocol of intermittent elevation of SVC perfusion pressure to 45 mmHg every 30 seconds using near infrared oximetry for cerebral protection (Table 3) [52,53].
The approaches of total body retrograde perfusion by Yasuura and associates and combined antegrade cerebral perfusion with retrograde IVC perfusion at moderate hypothermia may hold promise, because it allows precise control of perfusion flow and pressure in the brain and simultaneously maintains blood flow to vital organs during anastomosis [59-61]. Using “Warmer” temperature can reduce the duration of CPB and perturbation of coagulate function. The safety and efficacy of this technique should be tested in a randomized controlled trial (Table 4).
Combination strategy of retrograde and antegrade cerebral perfusion
In 2019, Kanda and colleagues used a combination strategy of RCP at a flow rate of 100-300 ml/min at 20 mmHg followed by selective ACP of all arch vessels at 10 ml/kg/min to maintain the cerebral arterial pressure between 45-60 mmHg. Moderate hypothermia between 26°C and 28°C was induced on all 23 consecutive patients. They observed the cerebral circulation as measured by laser speckle flow meter (LSF) during SCP was significantly higher than simple circulatory arrest and RCP and concluded that cerebral micro circulation may not be adequate during RCP compared with SCP under moderate hypothermia (Table 5) [169].
Retrograde cerebral and distal aortic perfusion
In 1995, Bavaria JE and colleagues reviewed the results of the above technique on 156 patients undergoing elective and emergent operations of the thoracic aorta. They demonstrated that the addition of RCP decreased the stroke sate to 0% (p<001), and the mortality rate of 7.1% compared with 37% for HCA (p<0.005). The thoracoabdominal aortic operations, straight cross-clamping resulted in a 27% spinal cord injury and 24% renal failure. Addition of distal aortic bypass resulted in 7% reduction of neurological injury (p<0.01) and reduction of mortality from 22% to 7% (p<0.05) (Table 6) [135].
Spinal ischemia
With the use of deep hypothermia, an aortic arch replacement can be performed without ischemic injury to the spinal cord, abdominal organs and peripheral organs. However, while using a warmer core and higher ACP temperature, ischemic tolerance of other organs should be kept in mind.
In an attempt to analyse the effects of deep vs moderate (25-28°C) hypothermia on lower body ischemia, Kamiya and associates noted an overall paraplegia rate of 2.1% (8/377), but it was 18.2% (2/11) in patients with lower body circulatory arrest longer than 60 minutes [17]. Analysis of the published literature revealed that only one-third of the centres widely adopted some forms of distal or visceral perfusion during selective ACP. Thus, the safety margin for spinal ischemia during moderate hypothermic selective ACP may be less than widely assumed [170].
Concerns
Most studies reported in the literature and used for meta-analysis are retrospective observational studies demonstrating spectrum of beneficial, neutral, and detrimental effects of DHCA, ACP and RCP in humans and experimental models.
Evidences generated from retrospective observational studies are of lower quality than that from randomized control trials and have the potential for selection bias. Significant confounding factors (e.g. patient’s baseline status, preoperative disease, operation procedure, anesthesia management, CPB time, circulatory arrest time) were not always taken into account.
In most of the studies, there was absence of a consensus definition of transient neurological deficits after aortic surgery, non-availability of data on the degree of aortic atherosclerosis/calcification, extent and pathology of dissection, extent of arch replacement, preoperative neurological status and heterogeneous surgical expertise and techniques.
Despite statistical adjustment and the use of network met-analysis, the presence of unmeasured confounders and possible treatment allocation cannot be excluded. Therefore, the present studies should not be used to reach conclusive recommendations but can only be used to generate hypotheses for future higher-level clinical trials. As RCP has been recently supplanted by ACP, the retrograde cerebral perfusion data were from a historical era, therefore confounding analysis because of improvements over time.
Conclusions
We conclude that the literature remains divided on whether adjunctive ACP or RCP provides greater neuro protection and reduction of surgical risk. The benefit associated with the use of adjunctive antegrade or retrograde cerebral perfusion increases with the duration of circulatory arrest (arrest time exceeding 25 minutes) and is not influenced by the arrest temperature or the use of unilateral or bilateral antegrade cerebral perfusion. Additional cannulation may add embolic risk for the patient. Antegrade and retrograde cerebral perfusion should be preferred to deep hypothermic circulatory arrest, especially in case of extended circulatory arrest time.
Despite the limitations of retrospective studies, the general consensus of the meta-analyses is the following: i) both antegrade and retrograde cerebral perfusion are associated with significantly lower postoperative stroke, permanent neurological deficit and operative mortality rates in both elective and non-elective setting. The added complexities of aortic vessel manipulations for antegrade cerebral perfusion and perfusate delivery require institutional experience.
Dichotomous reports espouse the benefits of using deep versus moderate or even mild hypothermic circulatory arrest during prolonged surgeries of the aortic arch. Meta-analysis of hypothermic circulatory arrest alone vs hypothermic circulatory arrest with adjunctive retrograde cerebral perfusion indicated that in comparison to hypothermic circulatory arrest alone, adjunctive retrograde cerebral perfusion may reduce mortality and permanent neurological deficit with comparable incidence of transient neurological deficits.
Exploring the Unknowns: Future Directions
The communication is not meant in any way to convince those surgeons satisfied with their own methods of cerebral protection in high-risk patients undergoing arch reconstruction requiring prolonged circulatory arrest times. Due to limitation in the quality of the meta-analyses, older age of some studies, improvement in surgical techniques, the conclusions should only be used as a guide.
To properly test the hypothesis that antegrade and retrograde cerebral perfusion provide comparable outcome in patients undergoing deep hypothermic circulatory arrest, a multi-institutional registry focussing on surgical strategies, outcomes, collaborative pooling of raw patient data enabling risk stratification and propensity matching will serve as a better powered platform in lieu of randomized controlled trials and would be the last refute who cannot accept the conflicting complex findings of the published literature on the issue of cerebral protection. This will require longer studies such as those proposed by the International Aortic Arch Surgery Study Group to fully investigate this challenging question [171].
How to Cite
References
URL: https://www.annalsthoracicsurgery.org/article/0003-4975(92)90432-4/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/13274273
URL: https://www.ncbi.nlm.nih.gov/pubmed/6003480
URL: https://www.ncbi.nlm.nih.gov/pubmed/14026185
URL: https://www.ncbi.nlm.nih.gov/pubmed/14425176
URL: https://www.ncbi.nlm.nih.gov/pubmed/1186283
URL: https://www.amazon.com/Cardiovascular-Vascular-Disease-Aorta-Svensson/dp/0721654266
URL: https://www.annalsthoracicsurgery.org/article/S0003-4975(10)60643-1/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/3269219
URL: https://www.ncbi.nlm.nih.gov/pubmed/21747050
URL: https://www.ncbi.nlm.nih.gov/pubmed/21747050
URL: https://www.ncbi.nlm.nih.gov/pubmed/22099946
URL: https://www.ncbi.nlm.nih.gov/pubmed/14726038
URL: https://www.ncbi.nlm.nih.gov/pubmed/10391334
URL: https://www.jtcvs.org/article/S0022-5223(94)70334-5/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/17258589
URL: https://www.ncbi.nlm.nih.gov/pubmed/11216771
URL: https://www.ncbi.nlm.nih.gov/pubmed/8215684
URL: https://www.ncbi.nlm.nih.gov/pubmed/16311969
URL: https://www.ncbi.nlm.nih.gov/pubmed/19114203
URL: https://www.ncbi.nlm.nih.gov/pubmed/19549051
URL: https://www.ncbi.nlm.nih.gov/pubmed/9205156
URL: https://www.annalsthoracicsurgery.org/article/S0003-4975(98)00533-5/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/21269650
URL: https://www.annalsthoracicsurgery.org/article/S0003-4975(98)01186-2/abstract
URL: https://www.ncbi.nlm.nih.gov/pubmed/3377576
URL: https://www.ncbi.nlm.nih.gov/pubmed/9271762
URL: https://www.annalsthoracicsurgery.org/article/S0003-4975(97)00746-7/fulltext
URL: https://journal.chestnet.org/article/S0012-3692(15)37134-8/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/8901741
URL: https://www.ncbi.nlm.nih.gov/pubmed/11093473
URL: https://www.ncbi.nlm.nih.gov/pubmed/1510530
URL: https://www.ncbi.nlm.nih.gov/pubmed/9451056
URL: https://www.ncbi.nlm.nih.gov/pubmed/11465234
URL: https://trialsjournal.biomedcentral.com/articles/10.1186/s13063-019-3319-2
URL: https://www.ncbi.nlm.nih.gov/pubmed/12019380
URL: https://www.ncbi.nlm.nih.gov/pubmed/7646092
URL: https://www.ncbi.nlm.nih.gov/pubmed/9852917
URL: https://www.ncbi.nlm.nih.gov/pubmed/11479507
URL: https://www.ncbi.nlm.nih.gov/pubmed/8678693
URL: https://www.ncbi.nlm.nih.gov/pubmed/1728241
URL: https://www.annalsthoracicsurgery.org/article/S0003-4975(99)00434-8/abstract
URL: https://www.ncbi.nlm.nih.gov/pubmed/9305198
URL: https://www.jtcvs.org/article/S0022-5223(94)70485-6/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/12022542
URL: https://www.ncbi.nlm.nih.gov/pubmed/16077400
URL: https://www.ncbi.nlm.nih.gov/pubmed/16798306
URL: https://www.ncbi.nlm.nih.gov/pubmed/17000307
URL: https://www.ncbi.nlm.nih.gov/pubmed/22498084
URL: https://cardiothoracicsurgery.biomedcentral.com/articles/10.1186/1749-8090-5-97
URL: https://www.annalsthoracicsurgery.org/article/0003-4975(93)91042-L/pdf
URL: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(00)02818-X/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/12683577
URL: https://academic.oup.com/cardiovascres/article/32/4/632/264490
URL: https://www.ncbi.nlm.nih.gov/pubmed/8542536
URL: https://www.ncbi.nlm.nih.gov/pubmed/1554277
URL: https://www.ncbi.nlm.nih.gov/pubmed/8197437
URL: https://www.ncbi.nlm.nih.gov/pubmed/10469976
URL: https://www.ncbi.nlm.nih.gov/pubmed/8037512
URL: https://www.annalsthoracicsurgery.org/article/0003-4975(95)00735-0/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/23977575
URL: https://www.ncbi.nlm.nih.gov/pubmed/29789153
URL: https://www.ncbi.nlm.nih.gov/pubmed/25735404
URL: https://www.ncbi.nlm.nih.gov/pubmed/29625501
URL: https://www.ncbi.nlm.nih.gov/pubmed/23142122
URL: https://www.ncbi.nlm.nih.gov/pubmed/25890664
URL: https://www.ncbi.nlm.nih.gov/pubmed/24332107
URL: https://www.ncbi.nlm.nih.gov/pubmed/24908350
URL: https://www.ncbi.nlm.nih.gov/pubmed/25439767
URL: https://www.ncbi.nlm.nih.gov/pubmed/28460021
URL: https://www.ncbi.nlm.nih.gov/pubmed/30902473
URL: https://www.jtcvs.org/article/S0022-5223(02)73434-X/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/9271761
URL: https://www.annalsthoracicsurgery.org/article/S0003-4975(97)00745-5/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/8267476
URL: https://www.jtcvs.org/article/S0022-5223(02)73434-X/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/9271746
URL: https://www.ncbi.nlm.nih.gov/pubmed/8321002
URL: https://www.ncbi.nlm.nih.gov/pubmed/9271750
URL: https://www.ncbi.nlm.nih.gov/pubmed/11426767
URL: https://www.annalsthoracicsurgery.org/article/S0003-4975(10)62733-6/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/7721923
URL: https://www.ncbi.nlm.nih.gov/pubmed/7431967
URL: https://www.ncbi.nlm.nih.gov/pubmed/6977074
URL: https://www.ncbi.nlm.nih.gov/pubmed/2229147
URL: https://www.ncbi.nlm.nih.gov/pubmed/8279908
URL: https://www.ncbi.nlm.nih.gov/pubmed/7715222
URL: https://www.ncbi.nlm.nih.gov/pubmed/7795314
URL: https://www.annalsthoracicsurgery.org/article/S0003-4975(96)00933-2/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/7549190
URL: https://www.annalsthoracicsurgery.org/article/S0003-4975(98)00805-4/fulltext
URL: https://pascal-francis.inist.fr/vibad/index.php?action=getRecordDetail&idt=6570162
URL: https://www.ncbi.nlm.nih.gov/pubmed/23977577
URL: https://www.ncbi.nlm.nih.gov/pubmed/24629218
URL: https://www.ncbi.nlm.nih.gov/pubmed/20667348
URL: https://www.ncbi.nlm.nih.gov/pubmed/30448484
URL: https://www.ncbi.nlm.nih.gov/pubmed/7034010
URL: https://www.ncbi.nlm.nih.gov/pubmed/7717572
URL: https://www.ncbi.nlm.nih.gov/pubmed/8523875
URL: https://www.nature.com/articles/pr2001226
URL: https://www.ncbi.nlm.nih.gov/pubmed/7739257
URL: https://www.ncbi.nlm.nih.gov/pubmed/9667301
URL: https://www.ncbi.nlm.nih.gov/pubmed/15111162
URL: https://www.ncbi.nlm.nih.gov/pubmed/13875762
URL: https://www.ncbi.nlm.nih.gov/pubmed/7739248
URL: https://www.ncbi.nlm.nih.gov/pubmed/22480393
URL: https://www.ncbi.nlm.nih.gov/pubmed/23266252
URL: https://www.ncbi.nlm.nih.gov/pubmed/26809425
URL: https://www.ncbi.nlm.nih.gov/pubmed/3221583
URL: https://www.ncbi.nlm.nih.gov/pubmed/6625738
URL: https://www.worldcat.org/title/arteriensystem-der-japaner/oclc/1333885
URL: https://www.ispor.org/docs/default-source/resources/outcomes-research-guidelines-index/interpreting-indirect-treatment-comparison-and-network-meta-analysis-studies-for-decision-making.pdf?sfvrsn=2bb9f7db_0
URL: https://www.bmj.com/content/343/bmj.d4909
URL: https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/s12874-017-0315-7
URL: https://www.ncbi.nlm.nih.gov/pubmed/10391330
URL: https://www.ncbi.nlm.nih.gov/pubmed/11241084
URL: https://www.ncbi.nlm.nih.gov/pubmed/24045075
URL: https://www.ncbi.nlm.nih.gov/pubmed/25262171
URL: https://www.ncbi.nlm.nih.gov/pubmed/25035412
URL: https://www.ncbi.nlm.nih.gov/pubmed/24800197
URL: https://www.ncbi.nlm.nih.gov/pubmed/8873735
URL: https://www.ncbi.nlm.nih.gov/pubmed/9605085
URL: https://www.ncbi.nlm.nih.gov/pubmed/9692436
URL: https://www.ncbi.nlm.nih.gov/pubmed/9104985
URL: https://www.ncbi.nlm.nih.gov/pubmed/7475199
URL: https://www.ncbi.nlm.nih.gov/pubmed/7475199
URL: https://www.ncbi.nlm.nih.gov/pubmed/29100641
URL: https://www.ncbi.nlm.nih.gov/pubmed/6973326
URL: https://www.ncbi.nlm.nih.gov/pubmed/686902
URL: https://www.ncbi.nlm.nih.gov/pubmed/12004260
URL: https://www.ncbi.nlm.nih.gov/pubmed/12173824
URL: https://www.ncbi.nlm.nih.gov/pubmed/8911834
URL: https://www.ncbi.nlm.nih.gov/pubmed/7609569
URL: https://www.ncbi.nlm.nih.gov/pubmed/7132404
URL: https://www.ncbi.nlm.nih.gov/pubmed/25052822
URL: https://www.ncbi.nlm.nih.gov/pubmed/23977577
URL: https://www.annalsthoracicsurgery.org/article/0003-4975(95)00130-D/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/9852920
URL: https://www.ncbi.nlm.nih.gov/pubmed/12683577
URL: https://www.jtcvs.org/article/S0022-5223(01)20608-4/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/7994097
URL: https://www.ncbi.nlm.nih.gov/pubmed/28844545
URL: https://www.ncbi.nlm.nih.gov/pubmed/7853879
URL: https://www.ncbi.nlm.nih.gov/pubmed/2229147
URL: https://www.ncbi.nlm.nih.gov/pubmed/11385378
URL: https://www.ncbi.nlm.nih.gov/pubmed/20417760
URL: https://www.ncbi.nlm.nih.gov/pubmed/17553687
URL: https://www.annalsthoracicsurgery.org/article/S0003-4975(02)04340-0/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/22575432
URL: https://www.ncbi.nlm.nih.gov/pubmed/21955469
URL: https://www.ncbi.nlm.nih.gov/pubmed/19632396
URL: https://www.ncbi.nlm.nih.gov/pubmed/9636903
URL: https://www.ncbi.nlm.nih.gov/pubmed/17670327
URL: https://www.ncbi.nlm.nih.gov/pubmed/22419180
URL: https://www.ncbi.nlm.nih.gov/pubmed/26363654
URL: https://www.ncbi.nlm.nih.gov/pubmed/23142122
URL: https://www.ncbi.nlm.nih.gov/pubmed/24507981
URL: https://www.ncbi.nlm.nih.gov/pubmed/16798193
URL: https://www.ncbi.nlm.nih.gov/pubmed/23471152
URL: https://www.ncbi.nlm.nih.gov/pubmed/18249127
URL: https://www.ncbi.nlm.nih.gov/pubmed/30605642
URL: https://www.ncbi.nlm.nih.gov/pubmed/23628950
URL: https://www.ncbi.nlm.nih.gov/pubmed/24296985