Abstract
While left ventricular thrombus (LVT) is commonly observed in patients with acute myocardial infarction or dilated cardiomyopathy, its occurrence as the initial presentation of arrhythmogenic cardiomyopathy (ACM) is extremely rare. Herein, we report the case of a 20-year-old male patient who presented with new-onset severe heart failure with reduced ejection fraction(HFrEF(, in whom a left ventricular thrombus was incidentally detected on echocardiography. Standard etiological investigations did not reveal any evidence of coronary artery disease or myocarditis. Electrocardiography revealed findings suggestive of ε waves, while CMR imaging demonstrated diffuse fibrofatty infiltration of both ventricles accompanied by subepicardial late gadolinium enhancement, culminating in a definitive diagnosis of ACM. Following anticoagulation and guideline-directed heart failure therapy, the thrombus completely resolved, accompanied by substantial improvement in cardiac function. This case highlights that among young patients presenting with new-onset heart failure and concomitant LVT, a high index of suspicion for ACM is warranted, with CMR playing a decisive role in establishing the diagnosis.
Keywords
Abbreviations
LVT: Left ventricular thrombus; ACM: Arrhythmogenic cardiomyopathy;
CMR: Cardiac magnetic resonance; LGE: Late gadolinium enhancement;
HFrEF: Heart failure with reduced ejection fraction;
INTRODUCTION
T Left Ventricular Thrombus (LVT) is a common complication secondary to acute myocardial infarction or dilated cardiomyopathy, typically in the setting of severe left ventricular systolic dysfunction [1]. Arrhythmogenic Cardiomyopathy (ACM) represents a hereditary myocardial disorder characterized by progressive fibrofatty replacement of the ventricular myocardium, which often initially manifests as ventricular arrhythmias or sudden cardiac death [2]. The initial presentation of ACM with heart failure and concomitant left ventricular thrombus is extremely rare. Herein, we report the case of a young adult patient in whom an incidentally detected LVT served as a pivotal clue leading to the diagnosis of ACM.
CASE PRESENTATION
Case-reporting
A previously healthy, 20-year-old male patient presented with a 3 day history of chest tightness and dyspnea and was categorized as NYHA functional class IV at the time of admission. His medical and family histories were unremarkable. On physical examination, blood pressure was 104/82 mmHg, heart rate was 86 beats per minute, and body mass index was 31.46 kg/m². Lung auscultation revealed clear breath sounds, and a systolic murmur was appreciated at the cardiac apex. Laboratory investigations demonstrated an NT-proBNP level of 4820 pg/mL, a D-dimer level of 1302 ng/mL, with cardiac troponin levels within the normal range. Initial transthoracic echocardiography demonstrated significant left ventricular dilatation, diffuse hypokinesis, a left ventricular ejection fraction of 22%, severe tricuspid regurgitation, and trace pericardial effusion. On follow-up echocardiography performed on hospital day 6, a hyperechoic mass like lesion was observed at the left ventricular apex, consistent with LVT. Given that this finding was highly inconsistent with the patient’s age, the primary clinical consideration was initially directed toward ischemic or dilated cardiomyopathy. However, cardiac enzyme levels remained within normal limits, and there was no evidence of acute coronary syndrome. Electrocardiography demonstrated subtle low-amplitude waves in the terminal portion of the QRS complex in leads V1–V3, raising suspicion for ε waves and prompting consideration of an underlying structural genetic cardiomyopathy [3,4]. Cardiac magnetic resonance {CMR) imaging subsequently demonstrated biventricular enlargement, trabecular disarray of the right ventricle, diffuse fatty infiltration involving the left ventricular free wall and right ventricular wall, subepicardial linear late gadolinium enhancement (LGE), as well as left ventricular apical thrombus—a constellation of imaging findings fully consistent with the diagnostic criteria for ACM [5 7]. Accordingly, a final diagnosis of arrhythmogenic cardiomyopathy was established, complicated by severe Heart Failure with Reduced Ejection Fraction (HFrEF) and LVT [8] (Figure 1, 2,3) (Table 1).
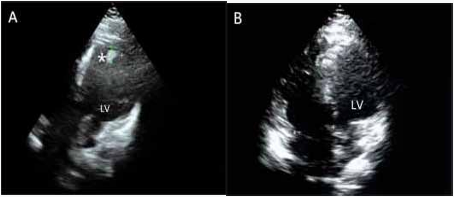
Figure 1: Serial transthoracic echocardiograms: (A) – The study was done at the index hospitalization showing a large thrombus at the left ventricular apex (asterisk) (B) - Follow-up evaluation subsequently demonstrated complete resolution of the left ventricular throm bus. LV: Left ventricle
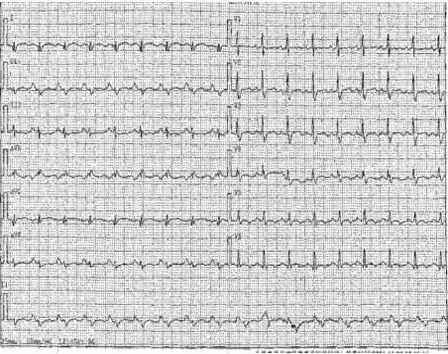
Figure 2: Electrocardiogram: Sinus tachycardia, 111 bpm heartbeat.
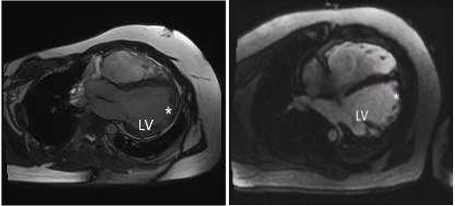
Figure 3: Delayed enhancement cardiac magnetic resonance imaging illustrates a thrombus measuring1.6cm*1.4cm (asterisk). Both im ages show an intracavitary thrombus within the LV apex (4-chamber views). LV: Left ventricle
Table 1: Padua criteria” for diagnosis of Arrhythmogenic Cardiomyopathy
|
Category |
Right ventricle (upgraded 2010 ITF diagnostic criteria) |
Left ventricle (new diagnostic criteria) |
|
By echocardiography, CMR or angiography: Major |
By echocardiography, CMR or angiography: Minor |
|
|
I . M o r p h o - f u n c t i o n a l ventricular abnormalities |
•Regional RV akinesia,dyskinesia, or bulging plus one of the following:-global RV dilatation (increase of RV EDV according to the imaging test specific nomograms)-global RV systolic dysfunction (reduction of RV EF according to the imaging test specific nomograms) |
•Global LV systolic dysfunction (depression of LV EF or reduction of echocardiographic global longitudinal strain), with or without LV dilatation (increase of LV EDV according to the imaging test specific nomograms for age, sex, and BSA) Minor |
|
Minor •Regional RV akinesia, dyskinesia or aneurysm of RV free wall |
•Regional LV hypokinesia or akinesia of LV free wall, septum, or both |
|
|
By CE-CMR: Major |
||
|
II.Structural myocardial abnormalities |
•Transmural LGE (stria pattern) of≥1 RV region(s) (inlet, outlet, and apex in 2 orthogonal views) By EMB (limited indications): Major •Fibrous replacement of the myocardium in ≥1 sample, with or without fatty tissue |
By CE-CMR: Major •LV LGE (stria pattern) of ≥1 Bull's Eye segment(s) (in 2 orthogonal views) of the free wall (subepicardial or midmyocardial), septum, or both (excluding septal junctional LGE) |
|
Major |
||
|
•Inverted T waves in right precordial leads (V1,V2, and V3) or beyond in individuals with complete pubertal development (in the absence of complete RBBB) |
||
|
Minor |
Minor |
|
|
I I I . R e p o l a r i z a t i o n abnormalities |
•Inverted T waves in leads V1 and V2 in individuals with completed pubertal development (in the absence of complete RBBB) |
•Inverted T waves in left precordial leads (V4-V6) (in the absence of complete LBBB) |
|
•Inverted T waves in V1,V2,V3 and V4 in individuals with completed pubertal development in the presence of complete RBBB. |
||
|
I V . D e p o l a r i z a t i o n abnormalities |
Minor •Epsilon wave (reproducible low-amplitude signalsbetween end of QRS complex to onset of the T wave) in the right precordial leads (V1 to V3) •Terminal activation duration of QRS ≥55 ms measured from the nadir of the S wave to the end of the QRS, including R', in V1, V2, or V3 (in the absence of complete RBBB) |
Minor •Low QRS voltages (<0.5 mV peak to peak) in limb leads (in the absence of obesity, emphysema, or pericardial effusion) |
|
V.Ventricular arrhythmias |
Major •Frequent ventricular extrasystoles (>500 per 24 h), non-sustained or sustained ventricular tachycardia of LBBB morphology Minor •Frequent ventricular extrasystoles (>500 per 24 h), non-sustained or sustained ventricular tachycardia of LBBB morphology with inferior axis (“RVOT pattern”) |
Minor •Frequent ventricular extrasystoles (>500 per 24 h), non-sustained or sustained ventricular tachycardia with a RBBB morphology (excluding the “fascicular pattern”) |
|
VI.Family history/genetics |
Major •ACM confirmed in a first-degree relative who meets diagnostic criteria •ACM confirmed pathologically at autopsy or surgery in a first degree relative•Identification of a pathogenic or likely pathogenetic ACM mutation in the patient under evaluation Minor •History of ACM in a first-degree relative in whom it is not possible or practical to determine whether the family member meets diagnostic criteria •Premature sudden death (<35 years of age) due to suspected ACM in a first-degree relative•ACM confirmed pathologically or by diagnostic criteria in a second-degree relative |
|
ACM = arrhythmogenic cardiomyopathy; BSA = body surface area; EDV = end diastolic volume; EF = ejection fraction; ITF = International Task Force; LBBB = left bundle-branch block; LGE = late gadolinium enhancement; LV = left ventricle; RBBB = right bundle-branch block; RV = right ventricle; RVOT = right ventricular outflow tract.
TREATMENT AND FOLLOW-UP
The patient was initiated on guideline-directed quadruple therapy for HFrEF, as well as anticoagulation using rivaroxaban 15 mg once daily [9-13]. At 1-month follow-up, echocardiography demonstrated complete resolution of the left ventricular thrombus, with LVEF improved to 30%. By the 7-month follow-up, the patient had achieved NYHA functional class I status, with LVEF having recovered to 44.6%. During this period, there were no episodes of thrombus recurrence or heart failure-related hospitalization. Although ICD implantation was repeatedly recommended [14,15], the patient declined this intervention at the time of the last follow-up.
DISCUSSION
The uniqueness of this case does not lie in ACM or LVT per se, but rather in the fact that left ventricular thrombus functioned as a pivotal clue to the diagnosis of underlying ACM. While ACM typically manifests initially as ventricular arrhythmias or sudden cardiac death [2], its initial presentation in the form of severe heart failure with concomitant LVT is exceedingly rare. In the present case, therefore, LVT was not simply a complication; rather, it served as a critical trigger that prompted further etiological investigation.
At advanced stages of ACM, extensive fibrofatty replacement of the myocardium results in significant impairment of left ventricular systolic function and ventricular dilatation. This pathological remodeling results in a markedly reduced blood flow velocity within the ventricular chambers, creating an environment of stasis particularly at the apex—a direct substrate for left ventricular thrombus (LVT) formation [16]. The present case demonstrates that the occurrence of LVT among ACM patients with severe left ventricular dysfunction is supported by a well defined pathophysiological basis [17], suggesting that this population may be at an elevated risk for systemic embolism.
Throughout the diagnostic process, echocardiography merely indicated the presence of heart failure and left ventricular thrombus, whereas CMR was essential in elucidating the underlying etiology. The presence of myocardial fatty infiltration and subepicardial linear LGE represents characteristic imaging features of ACM [18], a pattern distinctly different from those observed in dilated cardiomyopathy or myocarditis. In the present case, CMR not only confirmed the diagnosis but also fundamentally altered the understanding of the disease process, shifting the clinical perspective from “heart failure of unknown origin” to “advanced manifestation of genetic cardiomyopathy.”
Therefore, when young patients (particularly those <40 years of age) present with new-onset severe HFrEF and concomitant LVT in the absence of evidence of common etiologies, such as acute myocardial infarction, a high index of suspicion for underlying ACM should be maintained. Within this context, LVT can be regarded as an important imaging marker of advanced ACM. The timely use of CMR is of critical importance in establishing the diagnosis, performing risk stratification, and guiding subsequent sudden cardiac death prevention strategies.
CONCLUSION
Among young patients, left ventricular thrombus should not be regarded merely as a common complication of heart failure, but rather as a significant clue pointing to underlying genetic cardiomyopathy. The present case demonstrates that whenever severe left ventricular systolic dysfunction is observed in conjunction with LVT and no clear ischemic etiology is identified, the possibility of ACM should be actively entertained. The value of CMR in this patient population lies not only in thrombus confirmation but also in its unique capacity for tissue characterization, a feature that enables direct identification of ACM specific changes and facilitates early and precise diagnosis [6]. The timely recognition of ACM not only assists in the guidance of anticoagulation and heart failure management, but, more importantly, serves as an essential basis for the primary prevention of sudden cardiac death and for familial screening.