Abstract
Approximately 15% of patients undergoing Transcatheter Aortic Valve Replacement (TAVR) experience high-degree atrioventricular block (AVB) necessitating permanent pacemaker (PPM) implantation within the first 30 days post-procedure [1,2]. The frequency and severity of this complication, along with the effectiveness of treating it, underscore the importance of timely recognition and intervention. The issue of post-procedural conduction disturbances is further underscored by three key factors:
BACKGROUND
Approximately 15% of patients undergoing Transcatheter Aortic Valve Replacement (TAVR) experience high-degree atrioventricular block (AVB) necessitating permanent pacemaker (PPM) implantation within the first 30 days post-procedure [1,2]. The frequency and severity of this complication, along with the effectiveness of treating it, underscore the importance of timely recognition and intervention. The issue of post-procedural conduction disturbances is further underscored by three key factors:
1) A substantial number of patients experience conduction disturbances with unclear risk profiles regarding progression to complete heart block.
2) Optimal in-hospital and outpatient management of these disturbances warrants further investigation.
3) Advancements in pacing device technology have enriched electrophysiologists’ armamentarium, necessitating careful
selection of the most appropriate device based on each patient’s clinical characteristics. This review will outline the issue of conduction disturbances in the context of TAVR, present the current evidence-based approach to their management, and discuss potential future research directions.
PATHOPHYSIOLOGY
TAVR poses a risk of damaging the conduction system due to the close anatomical proximity of the bundle of His, the left bundle branch (LBBB), and the aortic valve. The bundle of His originates from the atrioventricular node, traverses the membranous part of the interventricular septum for a few millimeters, and then runs superficially along the lower part of the membranous interventricular septum until it bifurcates into the left and right bundle branches at the level of the aortic annulus [3]. The superficial course of both the bundle of His and the initial part of the LBB, along with their close spatial relationship with the aortic valve, make these areas vulnerable to mechanical damage from deploying the aortic prosthetic valve. Autopsy studies have shown that, in addition to direct mechanical compression, various forms of tissue damage such as edema, hemorrhage, and ischemia complicate the initial tissue trauma, contributing to post-procedural conduction system damage (e.g., complete heart block (CHB), LBBB) [4]. This could raise questions about the potential reversibility of the observed conduction disturbances. Clinically, the pathophysiological mechanism described above is confirmed by the increased frequency of conduction complications in certain clinical scenarios. A short membranous interventricular septum, a small diameter of the left ventricular outflow tract, the use of self-expanding valves, and the peri-procedural pre-dilation/ post-dilation of the aortic annulus have all been associated with a higher risk of AVB or LBBB, underscoring the importance of mechanical pressure exerted in this area [5-7]. The significant variability and unique anatomy of the area may play a crucial role in post-TAVR conduction disturbances. Previously, three major anatomical variants have been identified based on the course of the His bundle. In 50% of patients, the His bundle was relatively right-sided, in another 30% it was left-sided, while in approximately 20% of patients, the His bundle coursed under the membranous septum, just below the endocardium. The latter two phenotypes could increase the risk for conduction disturbances [8,9] (Figure 1).
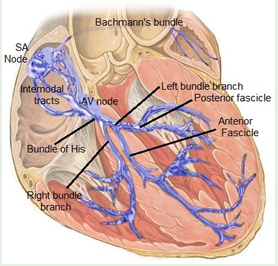
Figure 1:Close anatomical relationship between the conduction system and the aortic valve.
Screening considerations for TAVR patients
A structured approach to preprocedural planning and meticulous monitoring throughout the TAVR workflow, with attention to anatomical considerations and ECG findings, is essential for identifying and managing patients at risk of conduction abnormalities and PPM implantation. These predictors are categorized into preprocedural, intraprocedural, and post-procedural phases.
Pre-procedural Assessment
Before the procedure, CT heart-TAVR protocol is routinely obtained to assess the access vessel patency, further defines the aortic annulus anatomy and its relations to important surrounding structures such as the coronary arteries origins in the aortic root. Additional anatomical factors such as the length of the membranous septum, especially where the bundle of His exits, are critical, but rarely reported [10]. Compression in this area has been linked to higher rates of PPM implantation. Studies have demonstrated that the length of the membranous septum and its relationship to the depth of valve implantation are significant predictors of PPM implantation post-TAVR. The longer the membranous septum the higher the odds of post-TAVR conduction disrtubances [11,12].
Electrocardiogram
Baseline conduction disease is associated with higher risk for post-TAVR conduction complications. Up to 24% of patients with RBBB has been associated with increased rates of PPM implantation within 30 days post-TAVR (40.1% vs. 13.5%; p < 0.001). Similarly, patients with pre-existing first-degree AVB block or left hemi-block are also associated with a higher risk for conduction abnormalities during valve deployment [13].
Intraprocedural assessment:
During the procedure, for patients who are at high risk of conduction disturbances, the type of valve used should be carefully considered. An analysis was conducted on patient data retrieved from a national hospital administration database encompassing 49,201 individuals diagnosed with severe aortic stenosis. These patients underwent TAVR procedures using either Edwards Sapien Ballon expandable (BE) (Sapien XT and Sapien 3) or Medtronic Self-expandable (SE) (Corevalve and Evolut) bioprosthetic valves from 2010 to 2019 revealed that approximately 27% of the cohort underwent post-TAVR pacemaker implantation, with a majority occurring within the initial 30 days post-procedure. The rate of pacemaker implantation was slightly elevated among patients receiving SE devices compared to those receiving BE devices. Specifically, the difference was modestly higher in the Sapien XT group (Corevalve: hazard ratio [HR] 1.3 [95% CI, 1.21–1.4]; Evolut: HR 1.25 [95% CI, 1.21–1.34]) [14]. During valve deployment, several predictors have been associated with a high rate of pacemaker implantation: the development of LBBB, PR and QRS prolongation ≥20 milliseconds, and transient CHB are significant predictors of TAVR-related conduction disturbances. If a patient develops persistent complete heart block, transvenous pacing should be considered, with access via a secure temporary pacing lead before leaving the procedure room indicated [15-17].
Post-procedural assessment
Following TAVR, first-degree AV block alone may not independently predict the need for PPM implantation; changes in PR interval along with other factors should be carefully monitored. The management of new-onset LBBB post-TAVR remains contentious due to the absence of specific guidelines. LBBB is the most common conduction abnormality associated with TAVR, with an estimated frequency of 25%, though more recent studies report a frequency of 10.6-15% [18]. Depending on the timing of its occurrence post-procedure, LBBB can be categorized into three types:
1) Acute - occurring within 24 hours of the procedure, divided into periprocedural (85-94%) and postprocedural.
2) Subacute - detected after 24 hours but before discharge.
3) Late - presenting after discharge but within the first year post-procedure [19-21]. LBBB and PPM requirement: Although it is well-established that new-onset LBBB increases the likelihood of requiring a PPM, the frequency of pacemaker implantation varies significantly across studies (7-17%). Current data do not support the preemptive implantation of a pacemaker based on new-onset LBBB alone [18,22-25]. In the multicenter, prospective MARE study, 103 consecutive patients underwent implantable loop recorder implantation and were followed for one year. At the one-year mark, 20% of the patients experienced clinically significant bradycardia (high-degree AV block, severe bradycardia due to sinus node dysfunction), with approximately half of these episodes occurring within the first month. Eventually, half of these patients required a pacemaker, with the primary indication being the development of high degree AV block, and about half of the arrhythmic episodes were asymptomatic [26].
High-degree AVB or CHB: This is the most detrimental conduction disturbance post-TAVR, with a frequency estimated at 15% within the first 30 days post-procedure [27,28]. Newer data indicate that AV block reversibility is possible, necessitating special consideration, especially given the risk of pacemaker-induced LV function deterioration [29,30]. More data are needed to identify factors that reliably recognize patients at increased risk for delayed high-degree AVB
Similarly with post-TAVR new-onset LBBB, high-degree AV block occurs in most cases (60-96%) within the first 24 hours. Based on the duration, it can be further classified as transient or persistent; depending on whether it lasts more than 24-48 hours [31]. Previously, Kagase et al., demonstrated that the time of high-degree AV block onset influenced the rate of recovery. Defining recovery as transient high-degree AV block or as a ventricular pacing rate of less than 1% at 30 days, specifically, they demonstrated that early onset of high-degree AV block was associated with a higher likelihood of recovery, whereas delayed onset was linked to a reduced rate of recovery [32,33].
Monitoring
Patients may be eligible for early discharge within 24-48 hours if they do not have a primary pacemaker indication, have not developed new first- or second-degree atrioventricular AVB, have no new bundle branch block, and show no progression in their baseline first- or second-degree AVB or an increase in QRS duration of 10% or more. If any of these conditions are present, patients should remain on telemetry until their conduction is stable for at least 48 hours and should be discharged with an outpatient monitor for a minimum of 14 days [13,34-36]. Patients without QRS or PR interval prolongation within 48 hours post-TAVI, or those with pre-existing conduction abnormalities who experience QRS or PR interval prolongation >20 ms after the procedure, may be considered for ambulatory ECG monitoring or electrophysiology study [37-39]. If outpatient monitoring reveals new rhythm disturbances, such as atrial fibrillation, or worsening of baseline conduction disturbances, it is recommended that the patient continues using the monitor for at least 14 days after discharge [40].
Indication for pacing
Permanent pacing is currently recommended for patients experiencing complete or high-degree AVB persisting for 24-48 hours, or those with new-onset alternating bundle branch block following TAVR as outlined in the 2013 guidelines [41]. This recommendation contrasts with a strategy of clinical observation for up to 7 days to assess reversibility [42]. For patients with pre-existing RBBB who develop additional conduction disturbances during or after TAVR, early permanent pacing (immediately post-procedure or within 24 hours) is advised (Class IIa) [41,43]. Following TAVR, new onset LBBB is frequent due to anatomical proximity to the aortic valve. It is advised to monitor patients with new LBBB exhibiting QRS duration >150 ms or PR interval >240 ms, with extended in-hospital observation over 5 days recommended for those showing dynamic progression [44,45].
Role of electrophysiological studies (EPS)
The effectiveness of using EPS to guide PPM after TAVR has not been evaluated in a randomized prospective clinical trial. Notably, Toggweiler et al., reported that in a cohort of 1,064 patients who underwent TAVR, none of the 250 patients in sinus rhythm without conduction disorders developed delayed high-grade atrioventricular block (DH-AVB).34 Only one out of 102 patients with atrial fibrillation developed DH-AVB, and no patient with a stable ECG for at least two days developed DH-AVB. The authors suggested that patients without post-TAVR conduction disorders may not require telemetry monitoring, while all others should be monitored until their ECG is stable for at least two days [46,47]. Patients in the intermediate risk category (described earlier) are the most suitable candidates for EPS due to the uncertain pacing needs. Predictors for pacing necessity include new LBBB or new RBBB; PR interval increase of more than 20 ms with old or new LBBB; isolated PR interval increase of at least 40 ms; QRS duration increase of at least 22 ms in sinus rhythm, and atrial fibrillation with a ventricular response under 100 beats per minute in the presence of old or new LBBB.47 EPS Findings and their Implications for PPM Implantation: Rivard et al., found that an increase of at least 13 ms in the His-ventricular (HV) interval between pre- and post-TAVR measurements was associated with TAVR-related AVB. For those with new LBBB, a post-TAVR HV interval of at least 65 ms predicted subsequent AVB. The authors suggested that pacing is appropriate when these changes are identified on EPS, although a limitation of this study is the need for EPS before TAVR [48]. EPS-identified changes such as HV interval ≥75 ms (Tovia-Brodie et al.,) or ≥100 ms (Rogers et al.) may guide PPM implantation, though these studies lacked controls. A limitation of these studies is the absence of control groups, making it unclear what the outcomes would be without pacing [49-51].
Device Selection Post TAVR
Limited data have been published regarding the most suitable pacemaker type for implantation following TAVR, particularly among patients without a specific indication for bradycardia pacing. An observational study involving 85 participants explored the viability of His bundle pacing (HBP) in patients with new-onset persistent LBBB [52]. In this study, successful correction of LBBB was achieved in 11 patients (69%). In more than half of these cases, two ventricular leads were utilized, with the second lead positioned in the right ventricle (RV) or left ventricle (LV) via the coronary sinus (CS). Concerns with HBP in this context include the potential development of AVB or bundle branch block at a location distal to the site of His bundle capture following pacemaker insertion. Data are scarce on left bundle branch area pacing (LBBAP) for new-onset LBBB post-TAVR and primarily encompass small-scale studies involving individuals with conventional indications for pacing due to bradycardia (e.g. CHB) [53]. Information on cardiac resynchronization therapy (CRT) in this context is limited to isolated case reports [54]. In light of these limitations, the writing committee concluded that there is insufficient evidence to make definitive recommendations regarding the choice of device post-TAVR, except in cases involving AV block or LBBB in other clinical settings.
Long-Term Follow-up
The study, conducted by Corinne Marzahn, at the Heart Center Brandenburg in Bernau, focused on conduction recovery and the avoidance of permanent pacing after TAVR. The findings revealed that 45% of patients with pacemakers experienced recovery of intrinsic atrioventricular conduction after TAVR, consistent with observations from recent studies [55].
The PARTNER Trial (Placement of Aortic Transcatheter Valves) primarily investigated the safety and efficacy of transcatheter aortic valve replacement (TAVR) compared to surgical aortic valve replacement (SAVR) in patients with severe aortic stenosis. PARTNER trial highlighted that TAVR is associated with a higher incidence of conduction disturbances compared to SAVR, especially in terms of new-onset LBBB and the need for pacemaker implantation. While these conduction issues are concerning, they did not significantly affect overall survival, although careful patient selection and monitoring for conduction abnormalities are essential [56]. Post-hoc analyses of major TAVR trials like PARTNER and RECOVERY show that immediate mortality associated with these conduction disturbances may be low, long-term pacemaker dependence and ventricular dyssynchrony pose significant risks for heart failure and adverse outcomes [57].
Prognosis
Conduction abnormalities following TAVR are significant in predicting patient outcomes. Post-TAVR conduction abnormalities, particularly LBBB, have been associated with a higher risk of all-cause mortality and cardiovascular death. LBBB post-TAVR are more likely to experience left ventricular dysfunction due to the altered synchronization of ventricular contraction, leading to worsening heart failure over time left ventricular function and exacerbate heart failure [58]. Patients who develop complete heart block, experience a higher in-hospital mortality risk and longer hospital stay. Though pacemakers mitigate immediate risk, long-term reliance on pacing can lead to complications, including pacing-induced cardiomyopathy [59].
Future Directions
Future directions include randomized prospective clinical trials to assess the efficacy of EPS in guiding PPM after TAVR. This will help establish evidence-based guidelines and potentially reduce unnecessary PPM implantations. Developing consensus guidelines for the management of new bundle branch blocks and transient complete atrioventricular heart block post-TAVR should include risk stratification, monitoring protocols, and criteria for PPM implantation. Additional studies are needed exploring the role of advanced diagnostic tools such as cardiac magnetic resonance imaging (MRI) and newer electrophysiological mapping technologies to better understand the structural and functional changes in the conduction system pre- and post-TAVR.
CONCLUSION
Post-TAVR conduction complications are common and difficult to manage. Preprocedural planning and postoperative monitoring are essential to predict and identify high-risk patients. Management of new LBBB and transient AVB is particularly challenging. Finally, more data is needed regarding the device selection and EPS role in risk stratification.
How to Cite
References
URL: https://pubmed.ncbi.nlm.nih.gov/22587564/
URL: https://pubmed.ncbi.nlm.nih.gov/22625193/
URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6162790/
URL: https://pubmed.ncbi.nlm.nih.gov/19652115/
URL: https://pubmed.ncbi.nlm.nih.gov/26292585/
URL: https://pubmed.ncbi.nlm.nih.gov/31429947/
URL: https://pubmed.ncbi.nlm.nih.gov/30332419/
URL: https://pubmed.ncbi.nlm.nih.gov/24750717/
URL: https://pubmed.ncbi.nlm.nih.gov/28893961/
URL: https://pubmed.ncbi.nlm.nih.gov/20180918/
URL: https://pubmed.ncbi.nlm.nih.gov/32362173/
URL: https://pubmed.ncbi.nlm.nih.gov/26292585/
URL: https://pubmed.ncbi.nlm.nih.gov/33190683/
URL: https://pubmed.ncbi.nlm.nih.gov/31429947/
URL: https://www.researchgate.net/publication/347768020_851
URL: https://onlinelibrary.wiley.com/doi/10.1002/ccd.26666
URL: https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000000615
URL: https://pubmed.ncbi.nlm.nih.gov/27169577/
URL: https://pubmed.ncbi.nlm.nih.gov/24273252/
URL: https://pubmed.ncbi.nlm.nih.gov/23040577/
URL: https://pubmed.ncbi.nlm.nih.gov/31505615/
URL: https://pubmed.ncbi.nlm.nih.gov/32389906/
URL: https://pubmed.ncbi.nlm.nih.gov/25388650/
URL: https://pubmed.ncbi.nlm.nih.gov/31129090/
URL: https://pubmed.ncbi.nlm.nih.gov/30031719/
URL: https://pubmed.ncbi.nlm.nih.gov/22587564/
URL: file:///F:/JSM%20Central/Clinics/ClinicsCardiology/V3/D/CC-v3-1011/ClinicsCardiology-24-RW-1002.rar/researchgate.net/publication/371296981
URL: https://www.researchgate.net/publication/334153273
URL: https://pubmed.ncbi.nlm.nih.gov/31429947/
URL: https://pubmed.ncbi.nlm.nih.gov/23443735/
URL: https://www.researchgate.net/publication/334153273
URL: https://www.researchgate.net/publication/334153273
URL: https://pubmed.ncbi.nlm.nih.gov/27339844/
URL: https://pubmed.ncbi.nlm.nih.gov/23801822/
URL: https://academic.oup.com/europace/article/21/12/1851/5580342
URL: https://pubmed.ncbi.nlm.nih.gov/30093056/
URL: https://pubmed.ncbi.nlm.nih.gov/31431323/
URL: https://pubmed.ncbi.nlm.nih.gov/29406864/
URL: https://pubmed.ncbi.nlm.nih.gov/30031718/
URL: https://pubmed.ncbi.nlm.nih.gov/37283271/
URL: https://pubmed.ncbi.nlm.nih.gov/31118148/
URL: https://academic.oup.com/europace/article/21/12/1851/5580342
URL: https://pubmed.ncbi.nlm.nih.gov/31129090/
URL: https://pubmed.ncbi.nlm.nih.gov/38254339/
URL: https://pubmed.ncbi.nlm.nih.gov/27987072/
URL: https://pubmed.ncbi.nlm.nih.gov/25446155/
URL: https://pubmed.ncbi.nlm.nih.gov/28377313/
URL: https://pubmed.ncbi.nlm.nih.gov/32637116/
URL: https://pubmed.ncbi.nlm.nih.gov/27883975/
URL: https://pubmed.ncbi.nlm.nih.gov/7148708/
URL: https://pubmed.ncbi.nlm.nih.gov/38294976/
URL: https://academic.oup.com/europace/article/26/Supplement_1/euae102.419/7681184
URL: https://pubmed.ncbi.nlm.nih.gov/38695900/
URL: https://pubmed.ncbi.nlm.nih.gov/28893961/
URL: https://pubmed.ncbi.nlm.nih.gov/20961243/
URL: https://pubmed.ncbi.nlm.nih.gov/20308614/
URL: https://pubmed.ncbi.nlm.nih.gov/32313452/
URL: https://www.jacc.org/doi/10.1016/S0735-1097%2818%2931584-5