Abstract
Background: We sought to compare the outcomes of patients with multivessel CAD and Acute Coronary Syndromes (ACS) who underwent Coronary Artery By-pass Graft (CABG) and percutaneous coronary intervention (PCI) with or without intravascular ultrasound (IVUS) imaging.
Methods: We retrospectively reviewed all patients with MV-CAD and ACS who underwent CABG or PCI with or without imaging from 8/1/2018 – 7/31/2022 in a multicenter, single healthcare system. Baseline patient data, procedural characteristics, and patient outcomes were ascertained from a prospectively maintained institutional database. There were only 27 patients who met the “optimal imaging criteria”. These patients were imaged with IVUS pre- and post-PCI, had no dissections, no plaque burden greater than 50%, and a minimal lumen area of less than 5.0 mm2. The primary endpoint was one-year survival rate. The secondary endpoints were the one-year re-admission rate and one-year myocardial infarction (MI) event rate.
Results: Of 1,854 patients, 295 (15.9%) underwent CABG, 259 (14.0%) PCI with imaging, 1300 (70.1%) PCI without imaging, and only 27 (1.5%) met criteria for “optimal imaging” for PCI with IVUS. One-year all-cause mortality was significantly lower in CABG than in PCI with “optimal imaging” (p=0.0005). There was no significant difference between them in one-year readmission or one-year recurrent MI event rate.
Conclusions: Patients with MV-CAD and ACS had low use of intracoronary imaging overall. Despite the low denominator of accurately reported IVUS use in PCI, the optimal imaging group recorded only one adverse outcome. However, the low number of documented optimal imaging precludes definitive conclusions.
Keywords
Abbreviations: ACS
Acute Coronary Syndrome; CABG: Coronary Artery Bypass Graft Surgery; CAD: Coronary Artery Disease; IPTW: Inverse Probability Treatment Weights; IVUS: Intravascular Ultrasound; LOS: Length of Stay; MI: Myocardial Infarction; MM: Medical Management; MVD: Multivessel Disease; OCT: Optical Coherence Tomography; PCI: Percutaneous Coronary Intervention.
INTRODUCTION
Despite significant advances in revascularization strategies that have reduced morbidity and mortality rates in patients with multivessel Coronary Artery Disease (CAD) and Acute Coronary Syndrome (ACS), the optimal therapeutic approach remains uncertain. While randomized clinical trials and observational studies have demonstrated that coronary artery bypass grafting (CABG) offers superior long-term outcomes compared to Percutaneous Coronary Intervention (PCI) in patients with multivessel disease [1-5], the role of intravascular imaging during PCI remains less well defined. Intravascular Ultrasound (IVUS) and Optical Coherence Tomography (OCT) are increasingly utilized and recommended to guide lesion assessment and stent optimization [6-8], but their impact on outcomes compared with CABG has not been systematically studied. The present analysis compares clinical outcomes among patients with multivessel ACS who underwent CABG, PCI with intravascular imaging, PCI without imaging, or Medical Management (MM).
MATERIALS AND METHODS
We retrospectively reviewed all patients with multivessel CAD and ACS treated within a large integrated healthcare system between August 1, 2018, and July 31, 2022. Patients were stratified by treatment strategy: CABG, PCI with intravascular imaging (IVUS or OCT), PCI without imaging, or medical management. In addition to whether intravascular imaging was used, we also abstracted data on “optimal” imaging use, which was defined as imaging use pre- and post-PCI, stent-edge plaque burden less than 50%, no edge dissections, and minimal lumen area less than 5.0 mm2 [6]. Data were obtained from a prospectively maintained institutional database. Baseline demographics, comorbidities, and procedural characteristics were recorded.
The primary endpoint was one-year all-cause mortality. Secondary endpoints included one-year readmission, Myocardial Infarction (MI), and index hospitalization Length of Stay (LOS).
Sample characteristics are described using descriptive statistics. Frequencies and percentages are used to describe categorical variables. Means and standard deviations (or medians and ranges where appropriate) are used to describe continuous variables. Inverse probability treatment weights (IPTW) were created using the propensity scores from a logistic regression of treatment group onto age, sex, and the interaction between age and sex. The IPTW weights were calculated by inverting the estimated probability that each patient receives the treatment they received. Balance was assessed by examining the standardized difference of demographic and clinical variables before and after IPTW. Standardized differences between -0.1 and 0.1 are considered adequately balanced. Standardized differences are provided for all variables (except for outcome variables) for review, however only age and sex were checked for adequate balance. All regression models are weighted using the IPTWs. Generalized linear mixed models were performed for all outcomes with binary or count outcomes (MI, length of stay) with hospital site included as a random effect. All Cox proportional hazards models also include a random effect of hospital location. Statistical significance is determined by p < 0.05, and analyses were performed using SAS 9.4. (Figure 1,2).
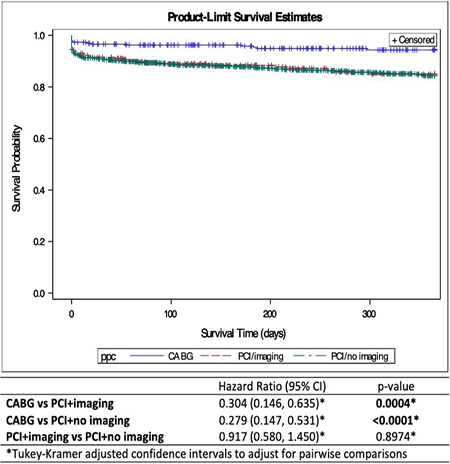
Figure 1: TAll-cause mortality within 1 year. A Cox proportional-hazard model with a random component to clustering within was per formed. CABG patients had significantly lower hazards of death compared to both PCI groups.
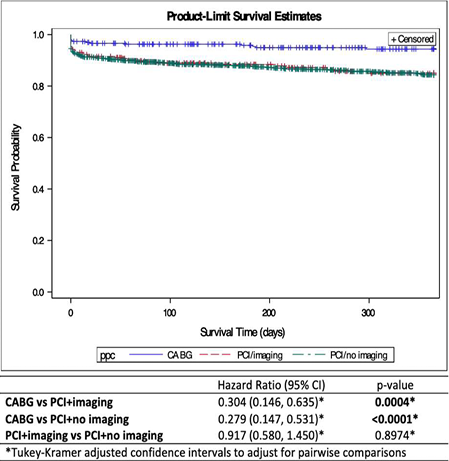
Figure 2: (Time to readmission in days within a year. A Cox proportional-hazard model with a random component to clustering within was performed. CABG patients had significantly lower hazards of readmission compared to both PCI groups, while there was no signifi cant difference in readmission between PCI patients who did and did not receive imaging.
RESULTS AND DISCUSSION
A total of 2,161 patients were included (CABG: 295 [13.7%], PCI: 1559 [72.1%], MM: 307 [14.2%]). CABG patients were slightly younger than PCI patients (65.8 ± 10 vs. 67.8 ± 12 years; p=0.002). Among PCI patients, 259 (16.6%) underwent PCI with intravascular imaging, while 1300 (83.4%) did not. Of those who underwent imaging with PCI, only 27 patients (1.5%) met the criteria for “optimal imaging” [6 - ULTIMATE trial].
One-year all-cause mortality was significantly lower among CABG patients compared with both PCI (HR 0.261, 95% CI 0.191–0.357, p<0.0001) and MM patients (HR 0.286, 95% CI 0.208–0.392, p<0.0001). There was no significant difference between PCI and MM (HR 0.914, p=0.57).
CABG patients also had significantly lower hazards of readmission compared with both PCI and MM patients. Median length of stay was longer with CABG (10 days, IQR 8–15) compared to PCI (3 days, IQR 2–6) and MM (3 days, IQR 2–5). At one year, CABG patients had lower risk of MI compared with PCI and MM (HR 0.357 vs PCI, p<0.0001).
Comparing PCI subgroups, outcomes were similar between PCI with imaging and PCI without imaging (Table 1).
Table 1: Baseline Demographics — CABG vs PCI with Imaging vs PCI without Imaging
|
Variable |
CABG/surgery (N=295) |
PCI/stent + Imaging (N=259) |
PCI/stent + No Imaging (N=1300) |
|
Age |
|||
|
Median (IQR) |
65.97 (59.73, 73.09) |
69.97 (62.22, 78.42) |
67.75 (59.95, 76.16) |
|
Min, Max |
34.55, 89.75 |
34.63, 96.75 |
26.69, 96.88 |
|
Mean (Std) |
65.78 (10.18) |
69.66 (11.85) |
67.48 (12.00) |
|
Sex |
|||
|
Female |
79 (26.78%) |
101 (39.00%) |
381 (29.31%) |
|
Male |
216 (73.22%) |
158 (61.00%) |
919 (70.69%) |
|
Race |
|||
|
American Indian or Alaska Native |
5 (1.69%) |
2 (0.77%) |
9 (0.69%) |
|
Asian |
12 (4.07%) |
15 (5.79%) |
54 (4.15%) |
|
Black or African American |
21 (7.12%) |
23 (8.88%) |
137 (10.54%) |
|
Missing |
0 (0.00%) |
0 (0.00%) |
1 (0.08%) |
|
Native Hawaiian or Other Pacific Islander |
1 (0.34%) |
1 (0.39%) |
2 (0.15%) |
|
Other |
1 (0.34%) |
1 (0.39%) |
6 (0.46%) |
|
Patient Declined |
2 (0.68%) |
2 (0.77%) |
2 (0.15%) |
|
Puerto Rican |
1 (0.34%) |
0 (0.00%) |
0 (0.00%) |
|
Some Other Race Only |
7 (2.37%) |
4 (1.54%) |
12 (0.92%) |
|
Unknown |
4 (1.36%) |
6 (2.32%) |
23 (1.77%) |
|
White or Caucasian |
241 (81.69%) |
205 (79.15%) |
1054 (81.08%) |
|
Height |
|||
|
Median (IQR) |
68.00 (65.00, 71.00) |
66.97 (64.00, 70.00) |
68.00 (65.00, 70.90) |
|
Min, Max |
55.00, 79.00 |
29.21, 76.00 |
24.41, 79.00 |
|
Mean (Std) |
67.73 (3.95) |
66.58 (4.75) |
67.57 (4.28) |
|
Weight |
|||
|
Median (IQR) |
190.00 (168.00, 219.50) |
176.38 (156.45, 208.31) |
188.06 (161.28, 220.00) |
|
Min, Max |
112.19, 350.06 |
78.94, 390.00 |
86.63, 456.38 |
|
Mean (Std) |
194.55 (39.33) |
183.10 (44.89) |
193.07 (46.17) |
|
BMI |
|||
|
Median (IQR) |
29.20 (25.90, 32.88) |
28.30 (24.60, 32.05) |
28.60 (25.68, 32.92) |
|
Min, Max |
19.50, 54.00 |
14.40, 55.90 |
15.80, 198.20 |
|
Mean (Std) |
29.69 (5.09) |
28.90 (6.14) |
29.76 (7.78) |
One-year mortality did not differ significantly (12.6% vs. 12.8%, p=0.93), nor did readmission (21.6% vs. 21.8%, p=0.93) or MI (3.7% vs. 3.6%, p=0.93). One-year all-cause mortality was significantly lower in CABG than in PCI with “optimal imaging” (p=0.0005). There was no significant difference between them in one-year readmission or one-year recurrent MI event rate.
DISCUSSION
In this large real-world cohort of patients with multivessel ACS, CABG was associated with lower one-year mortality, fewer readmissions, and lower MI rates compared with PCI or medical management, despite longer initial hospitalizations. These findings align with prior randomized trials and meta-analyses demonstrating superiority of CABG in multivessel CAD, including the BEST [9], trial and SYNTAX [3], analyses. Unfortunately, intravascular imaging did not impact PCI results compared to CABG, likely secondary to a low number of operators successfully performing or documenting “optimal imaging”.
When specifically examining PCI, the use of intravascular imaging (predominantly IVUS, with limited OCT utilization) did not result in measurable differences in mortality, readmissions, or MI compared with PCI performed without imaging. This finding may reflect several important limitations. First, while IVUS has been shown to improve stent expansion, optimize lesion coverage, and reduce stent thrombosis in controlled settings, the benefit is highly dependent on operator expertise and consistency in image acquisition and interpretation. In real-world practice across a large health system, IVUS may not have been systematically applied for optimization, and thresholds for minimal stent area or plaque characterization may not have been uniformly adhered to.
Second, the database may not have completely captured procedural details regarding whether IVUS was used simply for diagnostic purposes (lesion assessment, vessel sizing) versus for post-PCI optimization, which could dilute any observed benefit. Third, the proportion of patients undergoing imaging was modest (16.6% of PCI cases), and the study may have been underpowered to detect clinically meaningful differences between imaging-guided and angiography-only PCI (Table 2,3).
Table 2: Care group by imaging. Note that percentages are presented as the percent who did/did not receive imaging. An un weighted chi-square test was performed.
|
No imaging N=1860 |
Imaging N=301 |
p-value |
|
|
Group |
<0.0001 |
||
|
Medically managed |
281 (15.11%) |
26 (8.64%) |
|
|
CABG/surgery |
279 (15%) |
16 (5.32%) |
|
|
PCI/stent |
1300 (69.89%) |
259 (86.05%) |
Table 3: Outcomes by imaging. Note that percentages are presented as the percent who did/did not receive imaging. An un-weighted chi-square test was performed for categorical comparisons, and a Wilcoxon rank-sum test was performed to test the difference in length of stay
|
No imaging N=1860 |
Imaging N=301 |
p-value |
|
|
1-year Mortality |
0.9342 |
||
|
No |
1622 (87.2%) |
263 (87.38%) |
|
|
Yes |
238 (12.8%) |
38 (12.62%) |
|
|
Readmission within 1 year |
0.9275 |
||
|
No |
1454 (78.17%) |
236 (78.41%) |
|
|
Yes |
406 (21.83%) |
65 (21.59%) |
|
|
MI within 1 year |
0.9266 |
||
|
No |
1794 (96.45%) |
290 (96.35%) |
|
|
Yes |
66 (3.55%) |
11 (3.65%) |
|
|
Length of stay |
0.3260 |
||
|
Median (IQR) |
4 (2, 7) |
4 (2, 7) |
|
|
Min, Max |
0, 89 |
0, 46 |
|
|
Mean (SD) |
5.89 (6.74) |
6.08 (6.45) |
We know from prior work in the BEST trial in patients with multivessel coronary artery disease, the rate of major adverse cardiovascular events was higher among those who underwent PCI with Everolimus-eluting stents than with those who had undergone CABG [9]. Furthermore, recent subgroup analyses from this trial showed that in patients where the operators demonstrated optimal IVUS techniques outcomes were similar among PCI and CABG cohorts highlighting the importance of not simply utilizing IVUS but also utilizing it well. This notion was underscored with a recent meta-analysis on multi-vessel PCI and IVUS use demonstrating improved PCI outcomes, comparable to CABG, among the landmark clinical trials comparing the two revascularization strategies [7]. Unfortunately, the low rates of optimal imaging use here likely left any statistical comparisons underpowered.
Several limitations merit consideration. First, this was a retrospective analysis from a single integrated healthcare system, and treatment allocation was not randomized. Despite use of propensity weighting, residual confounding cannot be excluded [8-12]. Second, intravascular imaging was not uniformly applied, and our dataset did not capture critical details such as stent expansion indices, minimal stent area thresholds, or specific IVUS/OCT optimization strategies. Thus, imaging may have been used for lesion assessment alone in some cases, without systematic post-PCI optimization, potentially attenuating any observed benefit. Third, operator expertise and interpretation of IVUS are known to vary widely, and the lack of standardized protocols across centers may have limited the impact of imaging in this real-world setting. Fourth, the overall proportion of patients undergoing imaging was relatively low, reducing statistical power to detect outcome differences between PCI with and without imaging [13,14]. Finally, unmeasured confounders such as completeness of revascularization, surgical graft quality, and medication adherence could have influenced outcomes across treatment strategies.
CONCLUSION
Thus, CABG remains associated with superior one-year outcomes compared with PCI or medical management in patients with multivessel ACS. Intravascular imaging during PCI did not independently impact outcomes but also highlight the importance of rigorous implementation of IVUS and OCT, including standardized interpretation criteria, operator training, and integration with physiologic assessment. These findings support guideline-based recommendations favoring CABG in multivessel disease and emphasize the importance of proper intravascular imaging protocols and assessment when PCI is performed.
ACKNOWLEDGEMENTS
Funding for this work was generously contributed by the Baylor Scott and White Research Institute Cardiovascular Research Council Foundation.
How to Cite
References
URL: https://pubmed.ncbi.nlm.nih.gov/24240936/
URL: https://pubmed.ncbi.nlm.nih.gov/23439102/
URL: https://www.nejm.org/doi/full/10.1056/NEJMoa0804626
URL: https://pubmed.ncbi.nlm.nih.gov/22452338/
URL: https://pubmed.ncbi.nlm.nih.gov/30261237/
URL: https://pubmed.ncbi.nlm.nih.gov/39343665/
URL: https://www.ahajournals.org/doi/10.1161/CIR.0000000000001038
URL: https://www.researchgate.net/publication/369175739_Optimal_Intravascular_Ultrasound-Guided_Percutaneous_Coronary_Intervention_in_Patients_With_Multivessel_Disease
URL: https://pubmed.ncbi.nlm.nih.gov/27797291/
URL: https://pubmed.ncbi.nlm.nih.gov/27810312/
URL: https://pubmed.ncbi.nlm.nih.gov/26361150/
URL: https://pubmed.ncbi.nlm.nih.gov/23121323/