Abstract
We présent the case of a 62 year old woman who under went a percutaneous ballon valvuloplasty for bioprosthetic tricuspid stenosis. Percutaneous transcatheter ballon valvuloplasty is a developed technique that can be used to treat Tricuspid stenosis (TS), even if surgical tricuspid valve replacement remains the treatment of choice. Percutaneous Transcatheter Tricuspid ballon valvuloplasty (PTTBV) has been
performed in limited number of cases with favorable results.
The aim of this clinical case is to show that percutaneous transcatheter ballon valvuloplastyis a procedure that can be performed in Tricuspid Stenosis (TS) like aortic and mitral stenosis, to obtain transient improvement of symptoms and Tricuspid Stenosis before a definitive treatment.
Keywords
Introduction
Triscuspid bioprothetic valve stenosisis less common condition then aortic or mitral valve pathology.
Percutaneous transcatheter ballon valvuloplasty is a developed technique that has revolutionized the management of mitral stenosis [1], and can be used to treat Tricuspidstenosis (TS) although data on treatment of TS are limited.
We present a case report of a 62 year old woman who under went a percutaneous transcatheter tricuspid ballon valvuloplasty (PTTBV) for bioprosthetic tricuspid stenosis with temporary improvement in symptoms and tricuspid stenosis.
Case Report
A 62 year old woman presented with right sided heart failure symptoms encluding dyspnea, lower exteremity edema fatigue and ascites. She had a history of mitral stenosis since the age of 10. She had originally under gone mitral and aortic valve replacement at the age of 40, along with a tricuspid valve annuloplasty with a carpentier Edwards tricuspid ring for severe tricuspid regurgitation (TR). Ten year later she under went a tricuspid valve replacement with a bioprothesis due to persistant of severe tricuspid regurgitation. She remained a symptomatic until the age of 61, her fatigue increased and lower extreme tyedema worsened when she was admitted to hospital. The physical examination revealed signs of right heart failure of right heart failure. The patient was on atrial fibrillation. The echo cardiogram revealed severe thickened leaf lets of the bioprothetic tricuspid valve, with a severe tricuspid stenosis and mild regurgitation. The mean diastolic gradient across the tricuspid valve was 12 mmHg (Figure 2).
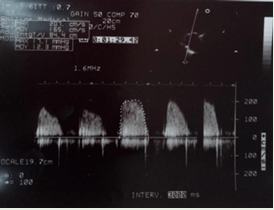
Figure 2: Transthoracic echocardiograms shows mean transvalvular gradients of 12 mmHg before valvuloplasty across the tricuspid valve.
We performed percutaneous transcatheter ballon valvuloplasty via the femoral approach, inflating an Inouie ballon n° 30mm (Figure 1). We use an inouie ballon because of our extensive experience in percutaneous valve dilatation with this device.
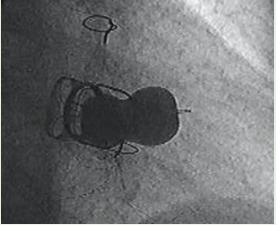
Figure 1: The inouie Ballon fully inflated across the bioprothetic tricuspid valve
According to hemodynamique measurements, once inflation was complete, the mean pressure gradient was reduced to 5 mmHg. The right atrial pressure dropped from 46 mmHg to 23mmHg. Post procedure transthoracic echo cardiography showed that mean gradient was reduced from 12 mmHg to 6 mmHg (Figure 3). The tricuspid régurgitation was inchanged. The patient tolerated the procedure well.
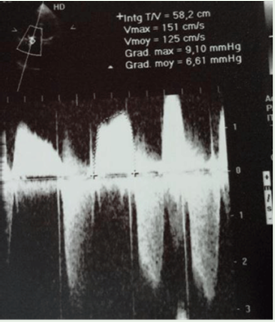
Figure 3: B: Mean graduent of 6 mmHg after valvuloplasty.
Six month later, the patient was readmitted to hospital because of dyspnea and peripheraledema, Transthoracic echo cardiography revealed moderate right ventriculardysfunction and recurrence of TS (Figure 4,5) with mild TR (Figure 4), we decided to perform PTTBV but we had to stop the preocedure due to uncrease of tricuspid regurgitation.
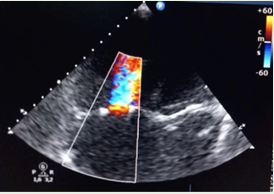
Figure 4: Color flow imaging in apical 4-chamber view shows the tricuspid stenosis jet, with enlargement of right ventricle
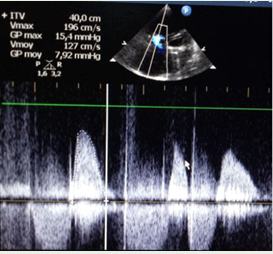
Figure 5: Tricuspid jet velocity recorded with continuous wave doppler with a mean gradient of 8 mmHg
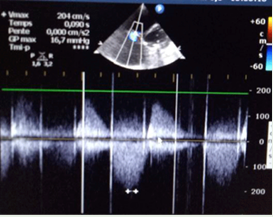
Figure 6: Mild tricuspid regurgitation
Discussion
Triscuspid bioprothetic valve stenosisis less common pathology then aortic or mitral valve stenosis. Percutaneous transcatheter ballon valvuloplastyis a procedure that can be performed to treat those cases. Severe tricuspid valve stenosisis associated with a mean gradient across the tricuspid valve of at least 5mmHG, a calculated TV area of less than 1.0 cm2 or both [2].
The 2014 AHA/ACC Valvular Heart Disease Guidelines recommends tricuspid valve surgery for patients with severe TS for both tricuspid bioprosthetic and native-valve stenosis, These class I recommendations are supported by level C evidence, and further suggest percutaneous balloon commissurotomy in patients with isolated, symptomatic severe TS with out accompanying TR [2].
The European Society of Cardiology (ESC) guidelines similarly recommend surgery for severe TS. Percutaneous balloon commissurotomy can be attempted as a first approach if tricuspid stenosis isolated [3].
There is a lack of data of patients with bioprothetic tricuspid valve stenosis receiving PTTBV, it has been performed in limited number of cases [4]. In this identified case reports, we noticed that there were improvement in mean pressure gradient and symptomatic benefits after PTTVB, but in some cases PTTVB failed, mostly because of the necessity of repeating the procedure or tricuspid valve replacement, with some patients who dies because of a pre-existing severe comorbid conditions such as sepsis [5-7].
Rana and collegues [8] presented case reports of 3 patients from their hospital experience, 2 of the 3 cases were successful with lasting clinical improvement, whereas the 3rd patient failed to show a reduction in valve gradient. They concluded that PTTBV should perhaps be considered for a selected patient population in which symptomatic improvement and hemodynamic stability are desired immediately, and particulary for patients who are in operable or at high surgical risk.
N Gaikwad and collegues [9] performed six ballons valvuloplasty in stenotic bioprosthetic tricuspid valve. Three of six cases were successful, 2 patients had recurrence of severe tricuspid stenosis and under went valve replacement. One patient with multiple comorbidities and shock died. They concluded that tricuspid valvuloplasty is an effective percutaneous procedure for the treatment of symptomatic bioprosthetic tricuspid valve stenosis.
There have been isolated case reports [10-12] suggesting that PTTBV is effective for stenosis of bioprosthetic tricuspid valve and associated with favorable results.
In our case, PTTBV improved symptoms and hemodynamic function of our patient. But the effect lasted only few months and we had to perform the procedure a second time because of recurrence of TS.
For our patient, PTTBV was an alternative to valve replacement since she had already two prior sternotomies. The aim was to produce a transient relief of symptoms and obtain hemodynamic stability before a definitive treatment.
Re operation has been the standard treatment for prosthetic valves that develop severe stenosis or regurgitation; But, repeat re intervention have a surgical risk, reaching and in-hospital mortality of 35% [13].
Transcatheter heart valve (THV) implantation with in a failed bioprosthesis, called “valve-in-valve” procedure, may offer a less invasive alternative. It has been successfully implanted by the transatrial, transjugular or transfemoral approaches [14,15] with two different THV: the EDWARDS SAPIEN valve and the Melody valve. The major complication associated with this technique is embolization of the valved stent in the right-sided cardiac chambers or pulmonary artery [17]. A few case reports and case series have documented outcomes in patients with tricuspid bioprosthetic valvular degeneration who under went valve in valve procedure [18,19], they concluded that THV is feasible and effective therapy for selected patients with failing bioprothesis in high surgical risk or in operable patients.
PTTBV can be an effective technique with low morbidity in selected patients. We believe that it can be considered as a transitional measure to improve symptoms in short term, especially when there is some temporary contra indications of Valve-in-valve procedure.
Conclusion
From this case, we conclude that PTTBV is reasonable option to consider as a bridge to eventual Valve in valve procedure, with the aim of effecting short term symptomatic improvement, especially if there is so me transient contra indications to performe Valve-in valve procedure, that is considered a promising alternative to redo surgery
How to Cite
References
URL: https://www.ncbi.nlm.nih.gov/pubmed/23180241
URL: https://www.ncbi.nlm.nih.gov/pubmed/24589852
URL: https://academic.oup.com/eurheartj/article/38/36/2739/4095039
URL: https://www.ncbi.nlm.nih.gov/pubmed/20329507
URL: https://www.ncbi.nlm.nih.gov/pubmed/1703459
URL: https://www.ncbi.nlm.nih.gov/pubmed/7517095
URL: https://www.ncbi.nlm.nih.gov/pubmed/24653745
URL: https://www.ncbi.nlm.nih.gov/pubmed/28265212
URL: https://www.heartlungcirc.org/article/S1443-9506(16)30752-1/fulltext
URL: https://www.ncbi.nlm.nih.gov/pubmed/17075017
URL: https://www.ncbi.nlm.nih.gov/pubmed/26424955
URL: https://www.ncbi.nlm.nih.gov/pubmed/24653745
URL: https://www.ncbi.nlm.nih.gov/pubmed/16077419
URL: https://www.ncbi.nlm.nih.gov/pubmed/26498535
URL: https://www.ncbi.nlm.nih.gov/pubmed/25172078
URL: https://www.ncbi.nlm.nih.gov/pubmed/26994123
URL: https://www.ncbi.nlm.nih.gov/pubmed/21251845
URL: https://www.ncbi.nlm.nih.gov/pubmed/25282331
URL: https://academic.oup.com/icvts/article/29/1/59/5301494javascript:;