Abstract
Objective: Tamponade and huge pericardial effusions are life-threatening entities, The goals of treatment may be simply to relieve symptoms (dyspnea), to put a diagnosis, to prevent recurrent effusion for a long-term symptomatic benefit, or to treat the local neoplastic disease with the aim of prolonging survival. We present our experience with pericardiodesis in 51 patients.
Material :During the last 10 years among 300 cases, only 51 patients with tamponade or large pericardial effusion were led to surgery. The main symptom was dyspnea and the diagnostic tools of choice were clinical examination and echocardiogram.
Results :All patients were submitted to pericardial window either thoracoscopically, or through a submammary3-4cm incision and in undiagnosed cases an additional lung and pleural biopsy were performed.A soft Foley catheter was introduced through the pericardial window as drainage and pericardiodesis with bleomycin was performed. Histology revealed in the majority of cases lung cancer. The postoperative course was uneventful. No recurrences were observed in a follow up of 5-10.2 months.
Conclusion :Pericardiodesis is an easy-to-perform and cost-effective method preventing from recurrences and offering even in end stage neoplastic disease a better quality of life.
Keywords
Introduction
The reported prevalence of pericardial diseases has changed over time and has varied according to diagnostic methods. Neoplasia and hematologic malignant diseases are the most common causes of acute pericardial effusionand tamponade. In an autopsy series, it has been found in 2%-4% of the general population, in 7%-12% of cancer patients and, among these, in 19%-40% of patients dying of lung cancer [1]. The presence of malignant pericardial effusion is associated with poor prognosis in these patients, with a shortened survival median time [2]. The goals of treatment may be simply to relieve symptoms (cardiac tamponade or dyspnea), to put a diagnosis, to prevent recurrent effusion for a long-term symptomatic benefit, or to treat the local neoplastic disease with the aim of prolonging survival. The best management for symptomatic MPE (surgical drainage vs. percutaneous pericardiocentesis [PCC]) is controversial and is based on local experience.
We present our experience in treating surgically malignant pericardial effusion producing tamponade along withpericardiodesis in 51 patients.
Material & Method
We reviewed all cases of massive pericardial effusion and cardiac tamponade that were admitted to our hospital during the last 10 years. Among 300 cases, only 51patients aged from 35-76 years were submitted to pericardial window, while the rest were simply drained by using the Seldinger technique. The main symptom they presented was increased dyspnea. Patients with acute tamponade also had tachycardia, and orthopnea, cough and chest pain. Cold and clammy extremities from hypoperfusion were also observed in some patients. Only in 14 cases (29%) there was a known history of neoplastic disease.
The EKG showed cardiac tamponade with sinus tachycardia, low voltage QRS complexes [Figure 1], while the chest x-ray revealed an enlarged cardiac silhouette and the “water-bottle” sign in the anteroposterior (AP), chest film [Figure 2].
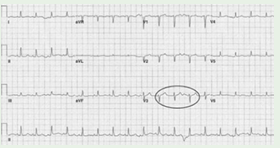
Figure 1: EKG showing cardiac tamponade with sinus tachycardia and low voltage QRS complexes.

Figure 2: Chest X-ray with enlarged cardiac silhouette.
Prompt diagnosis is always the key to reducing the mortality risk for patients with cardiac tamponade. Although echocardiography provides useful information, cardiac tamponade is a clinical diagnosis. Two-dimensional (2-D), echocardiography was used to visualize ventricular and atrial compression abnormalities as blood cycles through the heart [Figure 3]. CT scan was performed in some cases revealing prominent effusion both in thepericardiac and pleural spaces [Figure 4].
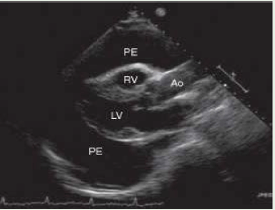
Figure 3: Two-dimensional (2-D) echocardiography visualizing ventricular and atrial compression abnormalities.
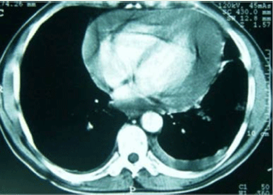
Figure 4: CT scan revealing prominent effusion both in the pericardium and pleural space.
All patients were led to surgery on an emergency basis. They were submitted to pericardial window either thoracoscopically, or through a submammary 2-3cm incision[Figure5]

Figure 5: Folley catheter introduced though the pericardial window.
Pericardium and pleural space were drained in all cases. The nature of effusion drained from the pericardial space was serous, haemorrhagic, or purulent. Fluids were sent to cytology, Ziehl-Neelsen staining, and Gram staining if purulent.The mean volume of fluid drained was 810mL. Pericardial biopsy was done in all cases and sent for histology. In undiagnosed cases an additional lung and pleural biopsy were performed. Additionally, asoft foley catheter was introduced through the pericardial window as a pericardial drainage.
Results
Cytology was positive in all but 6 cases, while histology revealed in the majority of cases lung cancer, in 4 breast cancer (7.8%), in 5 cases (9.8%) inflammatory disease and only in one tuberculosis. Extensive neoplastic involvement of the heart was found in one patient, while in 4 (7.8%), diffuse fibrofibrinous adhesion between the epicardium and pericardium were observed. In all cases pericardiodesis(instillation of an agent) was performed through the foley catheter in an interval of 72 hours postoperatively. At first, 2cc of xylocaine were instilled to avoid arrhythmias and then in cases of neoplastic disease a sclerosing- antineoplasticagent such as bleomycin (30-60 mg), while in cases of inflammatory diseases tetracycline was instilled. The postoperative course was uneventful resulting in complete control of the effusion in all cases.No recurrences were observed in a follow up of 10.5 months.
Comments
Massive pericardial effusion and cardiac tamponade are life-threatening cardiac pathologies that require urgent intervention. Tamponade occurs when all cardiac chambers are compressed as a result of increased intrapericardial pressure to the point of compromising systemic venous return to the right atrium (RA) [3].Increased intrapericardial pressure reduces the myocardial transmural pressure, and the cardiac chambers become smaller, with reduced chamber diastolic compliance and a decrease in cardiac output and blood pressure.The goal of treatment may be simply to relieve symptoms (cardiac tamponade or dyspnea), to prevent recurrent effusion for a long-term symptomatic benefit, or to treat the local neoplastic disease with the aim of prolonging survival. It is well known, that in developing countries, the dominant cause of massive pericardial effusion is tuberculosis, whereas in developed countries, it is more likely to be caused by cancer, infectious, iatrogenic, connective tissue diseases or idiopathic [4,5].
Various approaches have been proposed in order to avoid recurrences such as percutaneous drainage, pericardial window,sclerosing local therapy, local and/or systemic chemotherapy or radiation therapy depending also on the etiology. For instance, lymphoma and leukemias can be successfully treated with systemic chemotherapy, while for solid tumors, medical or surgical drainage and the use of systemic and/or local sclerosing and antineoplastic therapy seems to offer the best chance of success [1,6-10].
Since in our cases the majority of patients had an underlying malignancy, such as lung cancer, surgery seemed to be very useful in case of recurrences along with pericardiodesis. The surgical procedure we preferred was the creation of a pericardial window with a pericardial and a pleural drainage through a submammary incision of 3-4.5 cmor by Uniportal VATS. We avoided the subxiphoid approach because we did not want to spread cancer cells in the clean peritoneal cavity. Some authors support the idea that subxiphoid approach has an advantage over the thoracic approach, since it can be done in hemodynamically unstable patients under local anaesthesia. Also Uniportal VATS can be performed in an awake patient by using propofol, tramadol or dexmedetomidine, as it was done in 3 of our cases.
Cytology was not always proven positive in our cases in an urgent setting. On the one hand, reactive lymphocytes may be morphologically indistinguishable from malignant cells, while on the othermesothelial cells exhibit a spectrum of cytomorphologic features so the diagnosis might be ambiguous [11].
Chemical pericardiodesis has been used successfully to treat recurrent pericardial effusion due to malignancy. The authors performed pericardiodesis in all cases through a soft Foley catheter put intraoperatively in the pericardium. The larger diameter of the catheter proved to be more convenient for instillation of different agents without producing any arrhythmias. Noconstrictive pericarditis was observed.
Nowdays, the rationale of local chemotherapy is to obtain a higher local concentration of the antineoplastic drug. There have been very few pharmacokinetic studies performed on intrapericardial chemotherapy, but all confirm this hypothesis. In the literature, many different agents have been used, such as “pure” sclerosing agents, both sclerosing and antineoplastic activity (bleomycin or thiotepa), which seem to be quite effective, at least when associated with systemic chemotherapy. The immunomodulator OK-432 (a penicillin-treated powder) was used with many side effects and cytokines with low reported response [12-14]. Local chemotherapy with platinum, mitoxantrone and other agents are reported to produce a good local control of the disease, but the addition of systemic chemotherapy is probably relevant in order to prolong survival [15,16].
It is impossible to compare the efficacy of all these methods, because the diagnosis is often not well defined (large pericardial effusion in a patient with cancer classified as “malignant” even without cytology or neoplastic marker confirmation and the underlying disease is different in many reports) [1]. The survival rate ranges in medical and surgical series from 2.2 to 7.9 months [1,2,4,17], while in our surgical onereached 10.5 months.
In conclusion, the incidence of neoplastic pericardial disease and its prevalence among different primary tumors, have shown little change over time. It is more frequent in lung cancer patients. The diagnosis may be challenging and therapy should be limited to the control of symptoms in terminally ill patients only. Pericardiodesis is an easy-to-perform and cost-effective method preventing from recurrences and offering even in end stage neoplastic disease a better quality of life.
How to Cite
References
URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2999066/
URL: https://cardiooncology.onlinejacc.org/content/1/1/137
URL: https://www.nejm.org/doi/full/10.1056/NEJMra022643
URL: https://academic.oup.com/eurheartj/article/34/16/1186/452092
URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2931625/
URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2736808/
URL: https://pubmed.ncbi.nlm.nih.gov/11132262/
URL: https://pubmed.ncbi.nlm.nih.gov/2442107/
URL: https://pubmed.ncbi.nlm.nih.gov/2480244/
URL: https://pubmed.ncbi.nlm.nih.gov/7526307/
URL: https://onlinelibrary.wiley.com/doi/pdf/10.1002/clc.21952
URL: https://www.ahajournals.org/doi/full/10.1161/CIRCULATIONAHA.116.024041
URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2817063/
URL: https://pubmed.ncbi.nlm.nih.gov/8306816/
URL: https://pubmed.ncbi.nlm.nih.gov/15709087/
URL: https://pubmed.ncbi.nlm.nih.gov/12323163/
URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2658533/