Abstract
Post-myocardial infarction pericarditis, post-pericardiotomy syndrome and post-traumatic pericarditis are all under the ‘umbrella’ of postcardiac injury syndromes (PCIS). A traumatic event on the myocardium and/or pericardium can cause pericarditis with or without pericardial effusion, probably through an immune-mediated pathophysiological mechanism. Herein, we present a 73-year-old man who developed
pericarditis, while he was hospitalized at the cardiology clinic of another hospital, where he was diagnosed with mitral regurgitation due to chordae tendinae rupture. During the initial investigation, he underwent percutaneous coronary intervention (PCI). He was discharged and referred to cardiac surgeons for mitral valve repair. A few days later, he was admitted at the Internal Medicine Department due to low grade
fever. Pericardial effusion was found at computed tomography of the chest that was not present on the initial and repetitive ultrasounds of the former hospitalization. PCIS was the final diagnosis. Was the PCI or the chordae tendinae rupture of the posterior mitral leaflet the culprit?
Keywords
Introduction
PCIS are a group of syndromes where pericarditis develops after major or even minor cardiac injuries. Early post-myocardial infarction (MI) pericarditis and late post-(MI) pericarditis, also known as Dressler syndrome, along with post-pericardiotomy syndrome, are both the most recognized clinical conditions that connect cardiac trauma to pericarditis [1-3]. Nonetheless, recent case reports and case series do affirm that even minor cardiac procedures, such as PCI, pacemaker lead insertion and radiofrequency ablation increase the risk of developing PCIS; post-traumatic pericarditis. The more invasive the intervention, the more likely the PCIS is [4]. These procedures that include even minimal operation techniques (e.g. trans-septal puncture) and the simultaneous administration of anticoagulants, predispose to micro-perforations, hemorrhages and effusions [5]. Among the aforementioned categories, post-pericardiotomy syndrome has an incidence of 10-40% [6], while percutaneous coronary intervention has been associated with PCIS in less than 0.5% [7]. Importantly, post-traumatic pericarditis is not only associated with iatrogenic techniques. Non-iatrogenic causes; blunt (hitting the steering wheel of the car) or penetrating trauma may result to PCIS, too [8]. The pathophysiological substrate is incompletely understood, although immunological mechanisms have been implicated. The presence of anti-myocardial antibodies implicates the ‘’immune-mediated’’ concept; however, further data are needed to support this hypothesis [9]. The clinical picture is alike pericarditis of any cause; chest pain that is exacerbated by lying down and ameliorated by leaning forward, dyspnea and shortness of breath. Pericardial effusion may or may not be present, while an audible friction rub at the left lower sternal border is a strongly pathognomonic sign. Pleural effusions (pleuropericarditis) and/or pulmonary infiltrates have also been reported [10]. Female gender and pleura incision are two risk factors that predispose to pleuritic fluid accumulation. Electrocardiogram (ECG) is characterized by diffuse ST segment elevation with a down convex and PR segment depression, while in rare cases, such that of our patient, ECG can be normal. Cardiomegaly in chest-X-ray is noted when pericardial effusion is present. The fact that PCIS ‘responds’ to anti-inflammatory treatment with non-steroidal drugs (NSAIDs), colchicine and if needed cortisone, reinforces further the hypothesis of immunopathic process [11]. Our medical team recently encountered a 73-year-old patient with pericarditis.A week ago, he was hospitalized at the cardiology department of another tertiary hospital for mitral regurgitation due to chordae tendinae rupture. At that hospitalization PCI was performed. Almost ten days later, he was discharged from the hospital and medical instructions were given for surgical repair of the mitral valve. Two days after his discharge, he presented at the Internal Medicine Department complaining of low grade fever and subtle chest pain. Thorough investigation posed the diagnosis of post cardiac injury pericarditis.
Case Presentation
A 73-year-old man presented to the emergency department of our hospital due to new-onset low grade fever and chest pain that was aggravated in deep breathing. His past medical history included arterial hypertension, type 2 diabetes, dyslipidemia, macular degeneration and benign prostate hyperplasia. He was a former smoker, but had quitted before 35 years and drank alcohol socially. His current medication list was the following; perindopril 5mg, aspirin 100mg, rosuvastatin 5mg, tamsulosin 0.4mg once daily and metformin 1000mg twice daily. Two weeks prior his current hospitalization, the patient was admitted at the cardiology department of another hospital due to substernal chest pain. At that time, the electrocardiogram (ECG), showed sinus rhythm with no ST changes. Troponin levels were within normal range in sequential measurements.Transthoracic cardiac ultrasound displayed a left ventricle with normal dimensions and systolic function and a dilated left atrium. Mitral valve analysis showed first class chordae tendinae rupture of the posterior leaflet and flail into the left atrium with subsequent severe mitral regurgitation. The pericardial space was free of fluid. Transesophageal echocardiogram confirmed the above mentioned findings. Percutaneous coronary intervention was performed in the context of a preoperative investigation, since the patient was planned to undergo cardiac surgery for mitral valve repair. Angiographical significant stenotic lesions were not revealed, except for a 60% stenosis of the right coronary artery. The patient was discharged 11 days after his hospitalizationin order to immediately proceed with his mitral valve restoration.
Two days later, new onset of low-grade fever and substernal chest pain ‘brought’ the patient at the Internal Medicine Emergency Department. His vital signs were the following; blood pressure 110mmHg over 75mmHg, heart rate 75bpm, oxygen saturation 96% on room air and temperature of 37.80C. The patient was alert and oriented to time and place. Muscle strength and tone were normal. The cranial nerves were intact. The gait was steady and Romberg sign was absent. On cardiac auscultation, a holosystolic murmur at the apex was noted. S1, S2 were rhythmic. There was no jugular venous distention and no lower extremity edema. Lung auscultation was normal. Bowel sounds were present and there was no tenderness or rebound. There was no costovertebral angle tenderness. Skin examination revealed no exanthem or rash. 12-lead electrocardiogram showed sinus rhythm and non-specific ST changes [Figure 1]. The chest X-ray displayed an increase of cardiothoracic index [Figure 2].
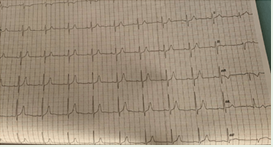
Figure 1: ECG with normal sinus rhythm, non-specific ST changes as repolarization abnormalities
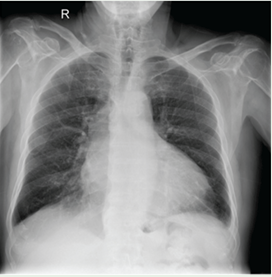
Figure 2: Patient’s chest-X-ray shows an increased cardiothoracic index
The abnormal laboratory findings were; WBC 9410 x 109 L (neut 81,2% lymph 9,5% mono 7,8%) Hb 10,8 g/dl Hct 33,9% Plts 442000 x 109 L, Ur 61 mg/dL Cr 1,3 mg/dL (eGFR 57 mL/min/1.73m2), SGOT 39 U/L SGPT 70 U/L C-Reactive Protein 206 mg/l. Polymerase chain reaction (PCR) for SARS-COV2 was negative. The patient was transferred to the floor and multiple blood cultures were obtained. Serologic testing was negative for varicella zoster (VZV), cytomegalovirus (CMV), Epstein-Barr (EBV), Herpes zoster (HSV), Toxoplasma and HIV. Tumour markers, rheumatoid factor, anti-nuclear antibodies and tuberculosis test were negative, too. Computed tomography of the chest revealed significant pericardial effusion [Figure 3-4].
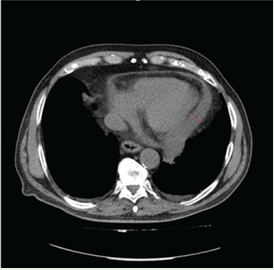
Figure 3: Chest CT showing the pericardial effusion (red double arrow)
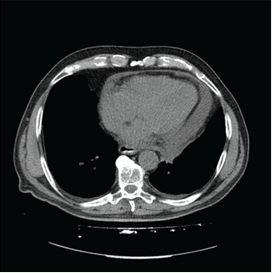
Figure 4: Chest CT showing the pericardial effusion (red double arrow)
The diagnosis of acute pericarditis was the working diagnosis. Since infectious (viral and bacterial), malignant, metabolic, drug-induced and chronic auto-immune diseases were excluded and given that this patient developed acute pericarditis after chordae tendinae rupture of the posterior mitral leaflet and PCI, it was concluded that PCIS was the final diagnosis.
Discussion
Hence, we initially encountered a patient with a known history of a recent chordae tendinae rupture who presented with low-grade fever. An initial thought was infective endocarditis; a patient with fever, an inflammatory syndrome (anemia, thrombocytosis, high CRP), and a pathological mitral valve. Thus, multiple blood cultures were initially obtained and antibiotic coverage was withheld, since the patient was not septic. However, the pattern of the fever was not compatible with that of bacterial endocarditis and further investigation was performed. On chest computed tomography, we realized that pericardial effusion was present. The patient, a few days ago, had undergone echocardiography (TTE and TEE), and no pericardial effusion was noted. At that time, he also did not fulfill other criteria for pericarditis; absent friction rub and a normal ECG. So, it was a ‘’nosocomial’’ pericarditis. Review of the literature disclosed that PCIS develops after any kind of injury to the myocardium and/or pericardium. Coronary intervention could possibly be the culprit, since the combination of minor trauma and microperforation along with anticoagulation treatment may lead to pericardial effusion [12]. Nonetheless, our patient prior to PCI also had an automatic chordae tendinae rupture resulting in mitral flail, possibly a result of myxomatous degeneration; all the other causes of chordae tendinae rupture, such as mitral valve prolapse, subacute endocarditis, rheumatic heart disease and genetic anomalies of connective tissue, were excluded [13].
Post cardiac injury syndrome is a medical definition for a group of cardiac conditions that many physicians are not familiar with, or may recognize a subset of them. PCIS embraces post-MI (Dressler’s syndrome), post-pericardiotomy and post-traumatic syndromes. The former two are well recognized, since their incidence is much higher, while the latter, post-traumatic syndromes may evade of clinical suspicion. Post-traumatic syndromes are either iatrogenic; endovascular procedures, pacemaker lead insertion and ablation of arrhythmias or non-iatrogenic; blunt or penetrating trauma [14].
It is of outmost importance to understand that even a blunt chest trauma during a car accident (hitting on the steering wheel) may present with the same clinical picture as the patient in this vignette, as the patient suffering a myocardial infarction or as the patient recovering from an open cardiac surgery [15]. The diagnosis of PCIS requires an injury of myocardium, pericardium and/or pleura tissue along with either pericarditis (pericardial effusion is not mandatory) or inflammatory syndrome, which cannot be attributed to other autoimmune or inflammatory disorder. The clinical signs and symptoms may be indolent to severe enough and PCIS’ progression may be either slow or rapid with constrictive signs and hemodynamic instability [16]. Most of the episodes, almost 2/3 are self-limited and relapse has been reported in a percentage of a 10-15%. Early therapy induces remission within 7 to 10 days and reduces the episodes of relapse by half. The appropriate treatment is NSAIDs administration and colchicine for relapses. Patients who have contraindications to NSAIDs are given corticosteroid therapy at a low dosage [17]. Our patient, due to the elder age, received corticosteroids and a week later, the effusion and the inflammatory markers had markedly subsided.
Conclusion
This case is original because our patient had two trauma insults on the cardiac muscle, chordae tendinae rupture and PCI. The fact that his primary hospitalization was complicated by pericarditis and all the other medical causes of pericarditis were excluded, both support the diagnosis of PCIS syndrome. PCIS should be suspected in every patient with a prior MI or cardiac traumatic-iatrogenic or non-iatrogenic- history, who presents with symptoms and/or signs of pericarditis.
How to Cite
References
URL: https://pubmed.ncbi.nlm.nih.gov/3189147/
URL: https://pubmed.ncbi.nlm.nih.gov/1618216/
URL: https://academic.oup.com/eurheartj/article/36/42/2921/2293375
URL: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(04)15648-1/fulltext
URL: https://pubmed.ncbi.nlm.nih.gov/1737407/
URL: https://pubmed.ncbi.nlm.nih.gov/20805112/
URL: https://pubmed.ncbi.nlm.nih.gov/19463510/
URL: https://www.tandfonline.com/doi/abs/10.1080/08916930290028166
URL: https://pubmed.ncbi.nlm.nih.gov/20177006/
URL: https://www.uptodate.com/contents/post-cardiac-injury-syndromes
URL: https://europepmc.org/article/med/17706808
URL: https://pubmed.ncbi.nlm.nih.gov/20207434/
URL: http://europepmc.org/article/MED/8458116
URL: https://pubmed.ncbi.nlm.nih.gov/16553111/
URL: https://pubmed.ncbi.nlm.nih.gov/12934774/
URL: https://pubmed.ncbi.nlm.nih.gov/2200931/