Abstract
Maternal paracetamol intake and fetal ductus arteriosus constriction or closure: A case series analysis" [1]. The researchers collected 25 cases reported in 12 papers in the literature which fulfilled the criteria for their
analysis. The objective was to establish a causal relationship between the ingestion of paracetamol and the closure or constriction of the ductus arteriosus (DA) using the World Health Organization Uppsala Monitoring Centre (WHO-UHC) causality assessment system, a tool designed to assess causality in case reports. According to the system´s tools, the ingestion of paracetamol and the ultrasound abnormalities described in
the case series, the researchers classified causality as: unlikely, possible, probable and certain.
Recently, an interesting short report was published entitled:
“Maternal paracetamol intake and fetal ductus arteriosus constriction or closure: A case series analysis” [1]. The researchers collected 25 cases reported in 12 papers in the literature which fulfilled the criteria for their analysis. The objective was to establish a causal relationship between the ingestion of paracetamol and the closure or constriction of the ductus arteriosus (DA) using the World Health Organization Uppsala Monitoring Centre (WHO-UHC) causality assessment system, a tool designed to assess causality in case reports. According to the system´s tools, the ingestion of paracetamol and the ultrasound abnormalities described in the case series, the researchers classified causality as: unlikely, possible, probable and certain.
- Unlikely: 1 case (a very long time interval since exposure and diagnosis not compatiblewith the pathophysiology)
-Possible: 9 cases (no preexposure normal fetal ultrasound described in the reports, and no normalization before delivery described)
-Probable: 11 cases (no preexposure normal fetal ultrasound, constriction during exposure with subsequent normalization after paracetamol exposure was stopped)
-Certain: 4 cases (normal preexposure fetal ultrasound findings, fetal ductus arteriosus constriction or closure during or shortly after exposuredescribed in the reports).
Twenty-four cases had a fetal echocardiogram showing indirect and direct signs of DA constriction. Indirect signs are those which, in the absence of obstruction of the right ventricular (RV) outflow tract, pulmonary artery or branches, absence of left obstructions (coarctation of the aorta) or extra-cardiac malformations (diaphragmatic hernia), show signs of increased RV pressures (this ventricle is systemic in fetal life, since it sends systemic output through the DA to the lower 2/3 of the body). These signs include: tricuspid regurgitation, RV or right atrial (RA) dilation, pulmonary trunk dilation, pulmonary regurgitation without valve abnormalities, RV hypertrophy not explained by other causes, and RV dysfunction. Less common signs include: poor pulsatility index, cardiomegaly and pericardial effusion, which are compatible with greater RV dysfunction. RVaneurysm, and severe tricuspid regurgitation with papillary muscle rupture have also been described [2,3]. In the article under discussion, some cases also reported pulmonary valve and tricuspid valve thickening.
Direct signs include: visualization of DA constriction or narrowing (hourglass image), or longitudinal constriction (Figure 1). Direct parameters using color Doppler show turbulence due to high velocities in the ductal arch and DA. Spectral Doppler parameters are: systolic velocity greater than 1.4 m/s and diastolic velocity greater than 0.3 m/s (these values increase with gestational age, reaching 1.8 and 0.5 m/s, respectively, in the term fetus), and loss of the normal Doppler pattern (Figure 2).
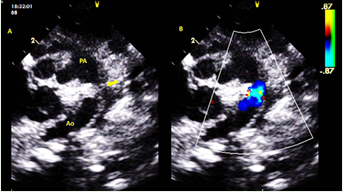
Figure 1: A: ductus arteriosus with zoom in fetal 34 weeks, yellow arrow shows ductus with constriction image. B: comparative color imagen shows aceletated flow in ductus arteriosus.
PA: pulmonary artery; Ao: desceding aortic.
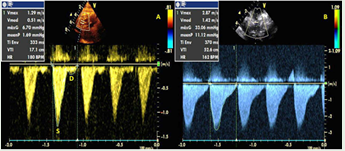
Figure 2: A: normal doppler espectrum in ductal arch in fetus 33 weeks. B: unnormal doppler espectrum in ductal arch, loss of normal waves, high velocities and increased gradients in fetus 36 weeks.
S: systolic wave; D: Diastolic wave.
Of the 24/25 cases with a fetal echocardiogram (fetal echo), only four had a previous exam which had explored the DA circulation and found it normal (classified as “certain”). The remaining 19 (classified as “possible” and “probable”) were performed due to a suspicion regarding the right chambers or fetal circulation (moderate tricuspid regurgitation, unexplained RV dilation, RV hypertrophy, acute fetal right decompensation, oligohydramnios, fetal distress, RV dysfunction, and dilated RA).The fetal echo exam showed the mentioned abnormalities of the DA and right chambers. Only one was ordered due to fetal arrhythmia, with the unexpected finding of DA constriction signs; the arrhythmia was interpreted as a sign of RV pressure overload. The paracetamol doses ranged from 1-4 grams per day (divided every 6-8 hours, just one, single dose of 1 gr/day), with cumulative times going from three days to two weeks of continual ingestion, just one, or intermittent doses. The main indication was pain management in 88% of the reports, and one case was self medication.
In fetal life, the DA represents one of the four important structures for regulating systemic cardiac output (placenta, ductus venosus, foramen ovale and DA) due to its contractile properties. The DA stays open due to low oxygen pressures and adequate levels of circulating prostaglandin E2 and I2, which are abundantly produced in the placenta and act on smooth muscle, keeping it relaxed and open [4]. On the other hand, the increase in vasoconstriction mediators such as thromboxane A2 and endothelin 1 and the increase in oxygen concentrations which normally occur in postnatal life are the causes of its natural closure [5].
The imbalance between dilation and constriction mechanisms in utero is a pathophysiological consequence which seriously affects normal DA hemodynamics, with consequences for the RV, pulmonary circulation and fetal cardiac output.
The history of paracetamol (acetaminophen in Anglo-Saxon countries) goes back more than one century. It is a derivative of aniline (phenylamine or aminobenzene), a toxic natural dye. Acetanilide was the first aniline derivative;its analgesic and antipyretic properties were discovered by chance, and it was introduced to medical practice by A. Cahn and P. Hepp in 1886, under the name “Antifebrin” [6]. Another derivative, known as phenacetin, was also used in 1887. Both compounds have toxic effects and cause cyanosis due to methemoglobinemia. In 1893, paracetamol was found in the urine of people who had ingested phenacetin, and in 1899 paracetamol was identified as a metabolite of acetanilide. This discovery was ignored at that time. However, long before, in 1873, Harmon Northrop Morse had already synthesized paracetamol at Johns Hopkins University through the reduction of p-nitrophenol with tin in glacial acetic acid, but this medication was not used for two decades. In 1887, the clinical pharmacologist Joseph Von Mering used paracetamol in patients, and in 1893 he published an article on the clinical results of paracetamol, finding that it had fewer methemoglobinemia production toxic effects than phenacetin. However, this research was disregarded, and paracetamol was ruled outfor therapeutic purposes.
Fifty years later, researchers in the United States in 1946, under the Institute for the Study of Analgesic and Sedative Drugs, awarded a grant to the New York Department of Health to study the problems associated with the use of analgesics. In 1948,Bernard et al. analyzed the metabolism of acetanilide and paracetamol, confirming that paracetamol is the main metabolite of acetanalide [7-9]. Finally, in 1949, Brodie et al. researched the metabolism of phenacetin, corroborating that it is also metabolized to paracetamol [10]. These studies led to the rediscovery of paracetamol as an analgesic and antipyretic medication, strengthening its marketing and sale in America and Europe.
However, more than 100 years after its discovery and use, its precise mechanism of action is still unknown. Between 1989 and 1992, Simmons et al. studied and identified two forms of cyclooxygenases which they termed cyclooxygenase-1(COX-1) and cyclooxygenase-2 (COX-2). These produce PGs from arachidonic acid, but their functions differ depending on the site and form of synthesis. Simmons established that PGs produced by COX-2 were responsible for fever, pain and inflammation, while those derived from COX-1 activity were gastric protectors and participated in the initiation of platelet aggregation. In an effort to find new, less toxic medications, they accidently discovered three new isoforms of cyclooxygenase derived from COX-1, which they named partial cyclooxygenase 1a (PCOX-1a), partial cyclooxygenase 1b (PCOX-1b) and cyclooxygenase 3 (COX-3) [11]. In 2002, Chandrasekharan published a study showing that acetaminophen effectively blocks the COX-3 isoform in experiments performed on canine cerebral cortex. In humans, according to Simmons, the expression of the COX-3 isoform is greatest in the cerebral cortex, spinal cord and heart [12].
For years, paracetamol has been considered to be a safe medication during pregnancy. As set forth by the authors of the article under discussion, fetal exposure to paracetamol is 37-53% [13,14]. It is mostly prescribed for pain management, which is very common at the end of pregnancy as a result of changes in the pelvic muscles and bones, due to fetal positioning. DA constriction in utero is greater after week 31, when it becomes more sensitive to the constriction factors.This coincides with many reports found in the literature. It is still not clear that paracetamol, whether in repeated or intermittent doses, prescribed by a physician or self-medicated in some cases, is 100% safe during pregnancy, especially at the end. The recommendations described by several authors are that as long as there is no researchedsafety margin regarding adverse effects of paracetamol at the end of pregnancy, fetal DA hemodynamics should be monitored using fetal echo when paracetamol is used.
For most reports in the study under discussion, changes in fetal circulation and DA reverted once paracetamol ingestion is stopped; almost all the cited studies showed this. Some of those cases were associated with the presence of congenital heart disease (CHD) (Tetralogy of Fallot, absent pulmonary valve and pulmonary valve stenosis) [15]. In my expert opinion, these cases are a coincidence, and their results should be interpreted with caution (classified as “possible” by the authors), since these types of conal trunk CHDs may be associated with DA agenesis.This has already been clearly described in the medical literature, and the finding is not surprising, even without paracetamol consumption [16,17]. Experimental models in rats have demonstrated the association between intravenous paracetamol exposure and DA constriction [18]. Studies in humans are difficult to perform due to the ethical implications of carrying out an exposure study. However, with the growing number of reports,research is expected on paracetamol pharmacodynamics.
What is clear is that whatever its mechanism of action, it has constrictive effects and the ability to closethe DA. It is not surprising that already in 2011, Hammerman et al. [19] reported the first cases of patent ductus arteriosus (PDA) closure with paracetamol in five premature infants. Since then, various clinical trials have shown the effectiveness of paracetamol for postnatal closure of DAs with hemodynamic repercussions in premature infants, showing aneffectivenesssimilar to that of non-steroidal anti-inflammatory analgesics (NSAIDs) [20]. Other clinical trials have also shown advantages compared to NSAIDs (decreased platelet aggregation, kidney failure, and hemorrhages, among others) [21]. One meta-analysis which included 14 studies with 454 premature infants having PDA with hemodynamic repercussions evaluated the effectiveness of oral vs. intravenous treatment, concluding that effectiveness was 77.79% for oral treatment and 81.52% for intravenous treatment (95% confidence interval for both) [22]. Paracetamol is safe for DAP closure even in very low weight premature infants, without the adverse effects described for NSAIDs [23,24]. Lastly, it has been used for DAP closure in clinical situations where NSAIDs have been contraindicated (high surgical risk, brain hemorrhage, thrombocytopenia) [25,26].
Conclusions
The study under discussion is the first to gather and analyze the causal relationship between paracetamol ingestion and DA closure or constriction in the largest case series. Of the 25 cases reported in the literature which meet the conditions for establishing the causal relationship in the study under discussion, 96% coincided with anatomic and functional abnormalities of the heart chambers and fetal circulation, seen on fetal ultrasound. These abnormalities may be present in other situations, such as CHD. Therefore, before making a conclusive diagnosis of DA constriction or closure in utero, they should be ruled outby a complete and detailed exam of the entire fetal cardiovascular system. Most cases resolve favorably, although some have presented pulmonary hypertension, cyanosis and respiratory distress in the immediate neonatal period, requiring hospitalization and medical treatments such as oxygen. In short and medium-term follow up, no sequelae have been reported. The DA is a vascular structure that must be perfectly balanced between dilation andconstriction mechanisms. While paracetamol is involved in DA constriction in utero, through the previously described mechanisms, this has further supported its use as an alternative medication for closure of PDAwith hemodynamic repercussions in premature infants, especially those with low weight and other comorbidities.The conclusion is that paracetamol may represent some risk for fetuses exposed in utero, especially at the end of pregnancy.At the same time, it has proven to be a useful medication for treating PDA with hemodynamic repercussion postnatally.Thus, this thought remains: paracetamol is “angel and demon”, depending on the circumstances in which it is administered.
Acknowledgement
To my daughter: D.Lynn. Thanksfor your support in this paper.
How to Cite
References
URL: https://www.ncbi.nlm.nih.gov/pubmed/30300944
URL: https://www.ncbi.nlm.nih.gov/pubmed/26443450
URL: https://www.ncbi.nlm.nih.gov/pubmed/28725980
URL: https://www.ncbi.nlm.nih.gov/pubmed/29941785
URL: https://www.ncbi.nlm.nih.gov/pubmed/18885610
URL: http://jpet.aspetjournals.org/content/94/1/29
URL: https://www.ncbi.nlm.nih.gov/pubmed/18885618
URL: https://www.ncbi.nlm.nih.gov/pubmed/18140117
URL: https://www.ncbi.nlm.nih.gov/pubmed/15317910
URL: https://www.ncbi.nlm.nih.gov/pubmed/12242329
URL: https://www.ncbi.nlm.nih.gov/pubmed/20659550
URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5648730/
URL: https://www.ncbi.nlm.nih.gov/pubmed/28745124
URL: https://www.ncbi.nlm.nih.gov/pubmed/1258771
URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4251345/
URL: https://www.ncbi.nlm.nih.gov/pubmed/27285464
URL: https://www.ncbi.nlm.nih.gov/pubmed/22065264
URL: https://www.ncbi.nlm.nih.gov/pubmed/26283668
URL: https://www.ncbi.nlm.nih.gov/pubmed/24359938
URL: http://www.jcnonweb.com/article.asp?issn=2249-4847;year=2018;volume=7;issue=3;spage=121;epage=124;aulast=Hossain
URL: https://www.omicsonline.org/open-access/paracetamol-for-the-treatment-of-patent-ductus-arteriosus-in-very-low-birthweight-infants-2167-0897-100e116.php?aid=76248
URL: https://www.ncbi.nlm.nih.gov/pubmed/29624206
URL: http://www.scielo.org.co/scielo.php?script=sci_abstract&pid=S0120-56332016000400020
URL: https://www.ncbi.nlm.nih.gov/pubmed/29043398