Abstract
Although catheter ablation is safe and effective in treating rapid arrhythmias, such as ventricular tachycardia and atrial fibrillation, there is a high recurrence rate after the first ablation in some patients. However, repeated catheter ablation increases the risk of serious complications. In addition, for patients with intractable arrhythmias whose underlying diseases are too many to tolerate invasive treatment or contraindications, there is an urgent need to develop a new non-invasive treatment paradigm. As a standard non-invasive targeted therapy for solid tumors, stereotactic body radiation has been gradually transferred to treat arrhythmias in recent years. At present, it is mainly used in treating ventricular arrhythmias and atrial fibrillation, which is called stereotactic arrhythmia radioablation under the guidance of electrocardiogram and imaging. The purpose of this review is to introduce the current situation and challenges in the treatment of ventricular tachycardia and atrial fibrillation, the basic concept, clinical experience, and critical issues of stereotactic arrhythmia radioablation, such as arrhythmia substrate mapping, dose selection, safety, and efficacy evaluation.
Keywords
INTRODUCTION
The potential anatomical structures that trigger and maintain arrhythmias may be congenital, just like bypass, formed during embryonic differentiation or the result of pathological changes such as myocardial infarction or scar formation after inflammation. Ventricular tachycardia (VT) is idiopathic or caused by abnormal myocardial substrate that induces arrhythmias and maintains re-entrant circuits [1]. The scar substrate is the most common after myocardial infarction, and the survival cardiomyocytes in the scar have poor coupling, slow and discontinuous conduction, which changes the typical conduction sequence of the heart [2-4]. In this case, re-entrant is the most common mechanism of VT [4]. The electrocardiogram (ECG) of this area showed separation potential, fragmentation potential, and late potential. For example, in patients with structural heart disease, myocardial scarring caused by infarction or alternative fibrosis is a common substrate for persistent monomorphic VT [5,6]. Compared with ischemic cardiomyopathy patients without VT, patients with VT demonstrated more significant endocardial low-voltage regions, higher density of scar-related ECG, and more conduction channels supporting VT [4]. This myocardial anatomical and electrophysiological disturbance lead to an independent and uncontrollable acceleration rhythm of the ventricle. VT is an abnormally rapid arrhythmia that is one of the leading causes of sudden cardiac death, with millions of people dying annually [7].
However, the mechanism of atrial fibrillation (AF) is more complex. The occurrence of AF includes two processes: triggering and maintaining. Triggering is that abnormal electrical activity initiates arrhythmia, while maintenance requires substrate in the sense of anatomy and electrophysiology [8]. The formation of the substrate is also the result of structural and electrical reconstruction. As the most common tachyarrhythmia, AF can be found in all age groups, leading to stroke, heart failure, and other serious complications, with a high rate of disability and mortality [9]. With the aging population and the aggravation of the burden of cardiovascular and other primary diseases, the incidence rate has an upward trend, which causes a tremendous economic burden to society [10]. The attack of Cardiac arrhythmia reflects the severity of heart disease and cardiac function. It indicates the decrease in patients’ Quality of life and the increase in hospitalization and mortality rates [Figure 1].
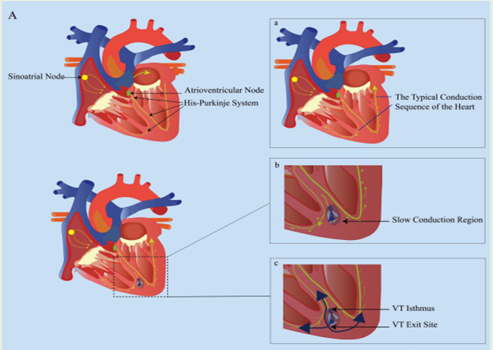
Figure 1: (A) Mechanism of VT; After myocardial infarction or inflammation, survival cardiomyocytes in the scar have poor coupling, slow and discontinuous conduction, and the dispersion of spatial repolarization is significant, which changes the heart’s typical conduction sequence and forms the re-entrant circuit. (a) The typical conduction sequence of the heart; (b) The slow conduction region after myocardial scarring caused by infarction or alternative fibrosis; (c) Formation of the re-entrant circuit in scar region..
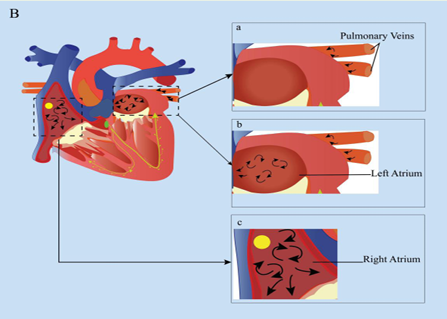
Figure 1: (B) Mechanism of AF; Abnormal electrical activation from the pulmonary veins triggers arrhythmia as an initiator, and the electrical and structural remodeling of the atrium provides a suitable substrate for the maintenance of AF. (a) Abnormal electrical activity from pulmonary veins; (b) and (c) support the maintenance of AF by providing the abnormal substrate.
CURRENT THERAPY AND CHALLENGES IN THE TREATMENT OF CARDIAC ARRHYTHMIAS
Current Therapy And Bottleneck Of Ventricular Tachycardia
Scar-mediated VT is a life-threatening arrhythmia. At present, the main treatment methods include antiarrhythmic drugs (AADs), implantable cardioverter-defibrillator (ICD), and catheter ablation (CA). At present, there are many kinds of AADs for ventricular tachycardia substrate. However, there is an increased risk of arrhythmia lacking curative effects with many side effects for most patients. Recurrent attacks of ventricular tachycardia can induce “electrical storm” promoting heart failure and increasing patients’ overall mortality. For ventricular tachycardia with hemodynamic instability and irreversible causes, ICD is both the first-line and the only life-saving treatment to save patients’ lives [11]. Although ICD can terminate ventricular tachycardia attacks by shocks, prevent sudden cardiac death, save patients’ lives, the painful process of ICD shocks, recurrent ventricular tachycardia, and frequent therapies with ICD decrease patients’ quality of life life [12-14].
CA mainly utilize radiofrequency or cryoablation to damage the myocardial tissue in direct contact or proximity to the tip of a catheter electrode, leading to tissue necrosis, changing or destroying the potential arrhythmogenic substrate. Sapp et al. [15], reported that the incidence of end-point death events, ventricular tachycardia storm, and ICD appropriate shocks in the catheter ablation group was lower than that of escalated antiarrhythmic drug therapy. During a mean (±SD) of 27.9 ± 17.1 months of follow-up, the primary outcome events occurred in 59.1% of the ablation group and 68.5% of the escalated-therapy group (hazard ratio in the ablation group, 0.72; 95% confidence interval, 0.53 to 0.98; P=0.04). Muser et al. [16], found that CA resulted in a significant reduction of VT burden, 45% of patients only took beta-blockers or no treatment, and 15% took sotalol or class I AADs, 22% only with amiodarone, which helped to reduce the related side effects of AADs.
Although CA has made remarkable progress in treating ventricular tachycardia, Sapp et al. [15], have found that the recurrence of VT after the first ablation approaches 50%. The success rate of ablation and the complication risks are highly dependent on the substrate targeted. Usually, the more extensive the range of the target tissue substrate means to the greater the possibility of tissue electrical conduction recovery and ventricular tachycardia recurrence after ablation [17]. In addition, it is also closely related to the location of the target tissue. The substrate deep in the endocardium, epicardial surface, or basal base is difficult to reach by traditional catheters, and the ablation effect is generally poor. When around the target tissue distribute essential structures, such as atrioventricular nodes, esophagus, phrenic nerve, or coronary artery, there is conductive myocardial tissue due to the relative lack of ablation energy the scar tissue after ablation [17]. These anatomical constraints and catheter ablation techniques limit the application of catheter ablation. Therefore, there is an urgent need to develop a new non-invasive treatment of refractory ventricular tachycardia.
Current Status and Challenges in the Treatment of Atrial Fibrillation.
At present, the treatment scheme related to AF mainly includes AADs and catheter ablation strategies. Among them, the efficacy of drugs for AF substrate and related complications is not satisfactory. Besides, there are some problems such as the high risk of side effects and heavy economic burden [18-20]. CA is the dominant treatment of medically refractory AF, and its primary goal is to form lasting electrical isolation circumferential pulmonary vein [18,21]. Although catheter ablation is a relatively safe and effective treatment, there is still a risk of potentially serious complications such as coronary vascular injury, pericardial tamponade, stroke, and atrioesophageal fistula [18]. Studies have found that the incidence of severe complications of CA is approximately 6% [22,23]. There is no doubt that repeated CA will increase the risk of these serious complications and increase the economic burden on patients and society.
THE BASIC CONCEPT OF STEREOTACTIC BODY RADIATION THERAPY
Stereotactic body radiation therapy (SBRT) commonly utilizes technology to treat solid tumors with precision and efficacy non-invasively. It delivers the radiation dose to the target tissue from multiple angles through three-dimensional reconstruction, image guidance, intensity modulation, and motion control. SBRT initially treated intracranial lesions using the Gamma Knife system. In the moving organs, the application of this technique is initially limited because it is challenging to locate the target tissue accurately. However, with the development of imaging, gating, tracking, and modulating the radiation beam’s intensity, SBRT has extended from intracranial lesions to other extracranial organs [24]. It began to be mainly used in treating patients with lung, liver, spine, prostate, and partially metastatic or inoperable tumors [25]. With the advent of the CyberKnife(CK) system, SBRT has achieved sub-millimeter precision and can theoretically target any part of the body [26]. The CK system can also directly track benchmark markers in or near tumors, provide high-precision treatment,and reduce radiation exposure to surrounding normal tissues and risk organs. SBRT is used widely, and new indications continue to appear. It gradually extends to treating nononcologic indications, such as trigeminal neuralgia, seizures, arteriovenous malformations, psychiatric, intractable anxiety [27,28]. Similarly, SBRT is also used to treat cardiovascular diseases such as renal artery hypertension and cardiac arrhythmia [29,30].
PRECLINICAL STUDY OF STEREOTACTIC BODY RADIATION THERAPY IN ANIMALS
When SBRT is used to treat cardiac arrhythmias, it is called stereotactic arrhythmia radioablation (STAR). First of all, a preclinical study was carried out in a healthy animal model to observe whether tissue fibrosis similar to catheter ablation can be produced by radiating specific structural tissues of the heart, such as atrioventricular node apical isthmus, pulmonary vein-atrial junction, and ventricular free wall. The time of fibrosis and electrophysiological changes in normal animal tissues after radiation were different, and most of them appeared 1-6 months after radiation [31,32]. In 2010, Sharma et al. [33] conducted animal model experiments in the CK system. It was found that electrophysiological alterations in the tricuspid isthmus, atrioventricular node, and pulmonary vein could be produced only after a single dose of 25Gy for more than four weeks, and there was no damage to surrounding organs, which preliminarily confirmed the feasibility of the formation of SBRT cardiopathy. One year later, Maguire et al. [34] delivered a single dose of 25-35Gy to irradiate healthy myocardial tissue in miniature pig experiments. Six months later, some pig models showed transmural fibrosis with electrical isolation.
Similarly, Blanck et al. [35], found that doses >32.5 Gy in the healthy pig heart model can induce transmural scarring of cardiac tissue non-invasively followed up for six months. In 2016, the Lehmann team [36] used 17 swines as experimental models to perform different ablation doses of atrioventricular node, right superior pulmonary vein, left atrial junction, and left ventricular free wall. The results showed that the lesion formation established a significant dose-response relationship for cardiac radiosurgery; a single dose of 25Gy produced slight fibrosis, 40Gy and 55Gy could produce significant fibrosis reaction, the left ventricular ejection fraction did not change significantly after six months of follow-up, and the ablation target tissue specimens showed vacuolization, fibrosis, and calcification. However, there is no radiation damage seen in surrounding tissues, and there was no change in the left ventricular ejection fraction.
CLINICAL STEREOTACTIC ARRHYTHMIA RADIOABLATION FOR CARDIAC ARRHYTHMIAS
Clinical Treatment Design
SBRT aims to combine computed tomography (CT), cardiac magnetic resonance imaging (CMRI), positron emission tomography (PET), electroanatomical mapping (EAM), and 12-lead electrocardiogram or electrocardiogram imaging (ECGI) to locate myocardial scar area and ventricular tachycardia re-entrant outlet. With the cooperation of cardiac electrophysiologists and radiation oncologists, we draw a three-dimensional model of substrate reconstruction target and guide the delivery system to target radiation to specific myocardial areas to destroy abnormal substrate and anatomy to reduce the burden of ventricular tachycardia. Unlike mediastinal tumor SBRT, which only considers the interference of respiratory movement, STAR also needs to consider the influence of cardiac contractile motion. In treatment planning and implementation, the strategy of limiting or compensating target movement is used to mark the protected area to reduce the damage to normal tissue and surrounding risk organs as much as possible. These strategies mainly include respiratory gating, that is, delivering radiation during a specific respiratory phase (such as during deep breathing), target tracking, that is, placing reference markers (opaque reference markers or external substitutes) near the heart target, potentially moving synchronously with the target, organ motion dampening, that is, reducing respiratory movement through abdominal pressure or breath-holding, and finally achieving precisely targeted delivering of the radiation beam to the target tissue.So far, STAR mainly applies to patients with the concealed substrate, heavy burden ventricular arrhythmia, the poor effect of traditional catheter ablation, and drug antiarrhythmic treatment or contraindications. Many case series in the literature have described the use of STAR in treating scar-mediated ventricular tachycardia or ventricular extrasystole, and the early feasibility study of STAR is encouraging. In current clinical studies, the median follow-up time of different series of ventricular tachycardia patients after STAR ranges from several months to several years, of which the longest is 28 months. Overall, STAR is safe and effective in the early treatment of ventricular tachycardia [Figure 2,3].
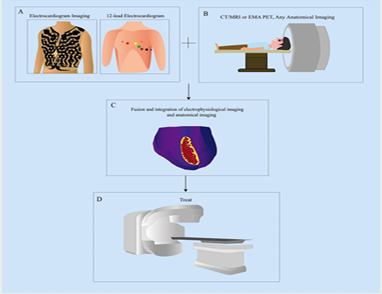
Figure 2: STAR work flow chart guided by electrophysiological and anatomical imaging: Through the dedicated software system, the images obtained from anatomical imaging such as CT, MRI, or EAM and the non-invasive electrophysiological mapping of ECGI or 12-lead ECG are co-registered to locate the myocardial scar area, delineate the three-dimensional target area and construct the ablation target volume; then, STAR is performed by the radiotherapy delivery system with the image guiding. The coincident area of red and yellow is the scar substrate that causes arrhythmia. (A) electrophysiological mapping; (B) anatomical imaging; (C) A and B locate the myocardial scar substrate; (D) delivery of STAR. CT: computed tomography; MRI: magnetic resonance imaging; EAM: electroanatomical mapping.
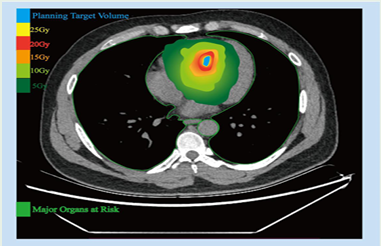
Figure 3: The conventional treatment regimen (25Gy prescription dose) with isodose lines in a single target. Light blue is the planning target volume, and light green is the surrounding major organs at risk (including lungs, aorta, esophagus).
Clinical Experience of SBRT for VT—Security
Previous SBRT experience of mediastinal tumors has shown that radiation-induced cardiotoxicity may not occur until several years later [37,38]. Basavaraju et al.[39], reported that the mean interval of radiation-induced heart disease after radiotherapy for mediastinal tumors is approximately 82 months, including valvular dysfunction and pericardial fibrosis pericardial effusion arrhythmias, decreased cardiac compliance, and diastolic dysfunction, with the pericardium being the most frequently involved. An autopsy study [40] on radiation heart disease found that 70% of cases had pericardial radiation diseases, including pericarditis, pericardial effusion, etc., especially pericardial effusion. At the same time, conduction system involvement was the most miniature, and the atrioventricular block was the most serious. In addition, radiation can also damage microvessels and large vessels, resulting in decreased capillary density, myocardial ischemia, fibrosis, and macrovascular injury, accelerating coronary atherosclerosis progression [37,38,41-45]. A study found that patients with mediastinal tumors had a 3.0 times higher risk of dying from fatal myocardial infarction than those without radiotherapy [42]; a meta-analysis included eight randomized trials found a more than 60% increase in cardiac mortality among women after radiotherapy [46]. Similarly, Hahn et al. [47], observed that after mediastinal radiotherapy in patients with Hodgkin’s lymphoma, the risk of advanced ischemic heart disease was correlated with radiation dose to the coronary artery.
Although the literature related to mediastinal tumor SBRT has described the late toxicity of cardiac tissue, the toxic effects of a single high dose of STAR on the heart’s local area are unknown. In theory, compared with traditional radiotherapy, STAR can be delivered with high precision under the guidance of images such as electroanatomical mapping. Its dose attenuation in all directions is better, avoiding cardiac substructure damage and minimizing toxic reactions. However, the phrenic nerve, esophagus, and lung may also be injured during STAR, and the degree of injury is related to radiation dose and sensitivity.
In the clinical study, Robinson et al. [48], enrolled 19 patients with refractory ventricular tachycardia in the ENCORE-VT study, with a median follow-up of 13 months. Among them, two patients had suffered grade 3 treatment-related adverse events within three months after the treatment, five patients experienced six treatment-related pericardial effusion, 3 cases were asymptomatic, 1 case was cured after treatment, and 2 cases were severe (including 1 case of grade 3 event and 1 case of grade 4 event). Two patients had radiation pneumonia confirmed by CT and were resolved with steroids. In addition, the standard grade 1-2 adverse events mainly included transient fatigue, dizziness, nausea, hypotension, and dyspnea. In 2019, the longer-term results of ENCORE-VT published by Robinson et al. [49], showed that STAR still had a persistent effect in most patients two years after the operation, and severe toxicity was low. However, near the end of follow-up, there was 1 case of pericardial effusion (grade 3 adverse event) at 2.2 years and one gastro-pericardial fistula (grade 4 adverse event, which needed surgical repair) at 2.4 years, which is acceptable for patients with heavy ventricular tachycardia, severe cardiac insufficiency, and short expected survival. However, it is still necessary to guard against the safety of long-term follow-up of STAR. Neuwirth et al. [50], found that during a median follow-up of 28 months, only one patient had a treatment- related grade 3 adverse event of mitral regurgitation. However, two patients died of heart failure and could not exclude the possibility that radiotherapy could promote the progression of heart failure.
At present, the maximum radiation tolerance dose of pacemaker and ICD is not precise, but so far, there are no reports of pacemaker or ICD damage caused by STAR. Nowadays, this new technique is mainly used for palliative therapy in patients with poor long-term survival rates. Long-term cardiac substructure and side effects of surrounding risk organs need to be followed up for a longer time in a larger population.
Clinical Experience of SBRT for VT—Efficacy
So far, the clinical study of STAR in ventricular tachycardia is only limited to small- scale prospective, retrospective case series, and case reports. In 2012, Loo et al. [30], treated an elderly male patient with STAR in the CK system for the first time. The scar was identified, and PET-CT reconstructed the target area. The maximum dose in the target center was 33Gy, with a dose fall off to 25 Gy at the margin of the scar. Seven months after the STAR treatment, ventricular tachycardia burden significantly decreased, and the use of AADs decreased. In 2014, Cvek et al. [51], also followed up an older woman who suffered from recurrent VT and arrhythmic storm in the CK system without any complications or malignant arrhythmia recurrence within the four months.
In 2017, Cuculich et al. [52], reported the first series of STAR cases. Five patients with high-risk and refractory ventricular tachycardia received a single dose of 25Gy(mean ablation volume of 49ml). The authors found that during the 6-week blanking period after ablation, there were a total of 680 episodes of ventricular tachycardia. However, in the following 46 months of follow-up, there are only four episodes of ventricular tachycardia, with a reduction of the burden by 99.9% from baseline. Among the four patients who survived for one year, three patients did not need to take ADDs. One patient received the fifth catheter ablation because of ventricular tachycardia recurrence four weeks after treatment, and one patient retook amiodarone nine months after treatment. The number of ICD shocks (55 before treatment vs. 1 after treatment) and the number of anti-tachycardia pacing (6577 before treatment vs. 3 after treatment) were significantly lower than those before treatment. Subsequently, Robinson and Cuculich registered a prospective phase I/II clinical study: ENCORE-VT (NCT02919618) to demonstrate further the short-term safety and preliminary efficacy of STAT in patients with refractory VT. In 2018, Robinson et al. [48], published the preliminary results of the first prospective trial, ENCORE VT, which enrolled 19 patients (17 for refractory ventricular tachycardia and 2 for premature ventricular contractions), with a single dose of 25Gy, median ablation time of 15.3min (range, 5.4-32.3min), and a median follow-up period of 13 months. Most of the patients were classified as II/III in New York heart function. The follow-up showed that the VT burden was significantly reduced, and the median number of VT episodes reduced significantly from 119 (range,4-292) before treatment to 3 times (range,0-31; P<0.001). VT burden was reduced by 75% in 89% of the patients. At the same time, it was observed that ICD shocks and anti-tachycardia pacing decreased. The median number of ICD shocks significantly reduced from 4 (0-30) to 0 (0-7), ICD anti- tachycardia pacing had a reduction from 81(range,0-292) to 3.5(range,0-29; P=0.001). While the ventricular tachycardia burden reduced significantly, ADDs also reduced, and the use of dual AADs reduced from 59% to 12% (P=0.008). For two patients with premature ventricular contraction (PVC) cardiomyopathy, the 24-hour PVCs burden reduced from 24% to 2%, 26% to 9%; and the left ventricular ejection fraction increased by 13% and 8%, respectively. The overall survival rate was 89% at six months and 72% at 12 months, of which three deaths were related to recurrence of ventricular tachycardia. At six months, 5 of the 9 ShortForm-36 areas suggested an improvement in Quality of life. In 2019, Robinson et al. [49], published the longer-term follow-up results of the phase I/II study. STAR still kept a persistent effect in most patients after the operation two years. However, two treatment-related adverse events included 1 case of grade 3 pericardial effusion and 1 case of grade 4 gastro-pericardial fistula. Immediately after, Lloyd et al. [53], published a STAR study of 10 patients with advanced heart failure, 2 of whom were eventually transferred to hospice care because of limited treatment. Regardless of the blank period, Out of the eight evaluable patients, seven were effective. The duration of ventricular tachycardia reduced 69%; after excluding one non responder, ventricular tachycardia was 94% lower than before treatment, and ICD shocks were reduced by 68%. Therefore, the authors believe that STAR is feasible in treating refractory ventricular tachycardia and has a specific effect on reducing ventricular tachycardia burden in patients with advanced heart failure.
In July 2019, Neuwirth et al. [50], published a retrospective case series of 10 patients with NYHA II-III grades. At the median follow-up of 28 months, and the VT burden was reduced by 87.5%. Nevertheless, in the end, there is a recurrence of VT in 8 out of 10 patients, and 2 of them had increased VT burden compared with the baseline, which shows that the curative effect of STAR has a downward trend with the prolongation of follow-up time. Similarly, in another prospective study reported by Gianni et al. [54], in August 2020, the STAR effect of five patients with VT was not satisfactory. Although there was no acute or early toxicity during the treatment, two patients died of late heart failure complications during the follow-up period. Despite the VT burden being less than before treatment during the first six months of follow-up, ventricular tachycardia recurred in all patients when the follow-up was one year. Three patients were treated with catheter ablation again, and surviving myocardial bundles were found in partially planned target volume scars. In the same year, Chin et al. [55], also reported limited efficacy of STAR. The cardiac function of 8 patients was NYHA (III-IV grade) with a mean ejection fraction of 21 ± 7% and a single dose of 15-25Gy. Although the median number of ICD treatments decreased from median 69.5 (45.5,115.8) to 13.3 (7.7,35.8; P=0.036), there was no significant difference in the reduction of VT (P = 0.24) after STAR 3 months. However, the authors thought that apparent clinical benefit occurred in 33% of patients after SBRT. There are significant differences in clinical efficacy among different research institutions, which could have been associated with the large target volume, long duration of operation, and severity of comorbidities in the non-responders compared with the series of cases with the good curative effect STAR reported by Cuculich et al.
In addition, STAR of life-threatening ventricular arrhythmia has been introduced into clinical practice. In May 2018, Jumeau et al. [56], reported the first case of severe incessant ventricular tachycardia with hemodynamic instability as a rescue treatment. STAR showed an immediate and persistent effect, and there was no recurrence of ventricular tachycardia during the 4-month follow-up period. Most importantly, the patient has left ventricular ejection fraction recovered. In 2020, Park et al. [57], also described the efficacy of STAR to ventricular arrhythmia induced by apical hypertrophic cardiomyopathy at the burnout stage. Catheter ablation was a failure because of the induction of hemodynamically unstable sustained monomorphic VT and ventricular fibrillation. A single dose of 24Gy divided into three fractions was delivered to the apical aneurysm. When there was no significant treatment- related toxicity, the antiarrhythmic effect was maintained for more than six months. The above cases indicate that STAR can be a rescue therapy for VT refractory to other treatment modalities.
Although clinical outcomes of 25 Gy single-dose SBRT for refractory VT remain limited to small prospective, retrospective cohort studies and few cases reports, STAR results are auspicious. It is expected that multicenter, prospective cohorts will be conducted in a larger population of patients to assess the long-term safety and efficacy of the STAR.
Clinical study of STAR in the treatment of Atrial Fibrillation
In 2016, Monroy et al. [58], reported the first real-world clinical study of robotic STAR in the treatment of pulmonary vein isolation. In this study, a patient with paroxysmal atrial fibrillation and a seven-year history chose STAR pulmonary vein isolation guided by CK system because the patient was concerned with the standard invasive catheter ablation, with a radiation delivery of approximately 35Gy. Although he developed permanent atrial fibrillation only six months after the procedure, there were no organ-related complications such as esophagus, pericardium, or lung during follow-up. One year after the operation, MRI showed that delayed enhancement could be observed around pulmonary veins, the base of the left atrial appendage, and the roof of the left atrium. However, whether the quantification of the MRI delayed enhancement region is helpful to modify the prognosis of STAR needs to be further discussed. This study confirmed for the first time the feasibility of STAR in the treatment of refractory atrial fibrillation. Subsequently, Qian et al. [59], performed STAR pulmonary vein isolation in 2 patients with refractory paroxysmal atrial fibrillation. The prescription dose of the myocardial target substrate was 25Gy, and the STAR plan was smooth without significant early or long-term side effects up during the 48-month follow-up period. Given the patient’s previous difficulty in rhythm control, all patients had received ADDs throughout the follow-up period. One did not develop persistent atrial fibrillation until six months, so he was converted to simple drug rhythm control therapy; the other found a little pericardial effusion without hemodynamic effects but maintained sinus rhythm at 24 months of follow-up. MRI showed that myocardial fibrosis was consistent with ablation lesion. Based on the closeness of the pulmonary vein to the adjacent anatomical structures (such as the esophagus), both papers [58-59] discussed the safety of STAR in the treatment of AF. Monroy et al. [58], focused on the esophagus, pericardium or lung during the follow-up period and found no significant damage. To minimize the radiation dose of the esophagus, Qian et al. [59], planned a pairwise wide-area circumferential ablation lesion set with a confluent overlap at the posterior wall. According to the currently published clinical studies, the short- term safety of STAR in pulmonary vein isolation treatment is satisfactory. However, more clinical studies are needed to evaluate the efficacy and long-term related complications further.
Mapping of Cardiac Arrhythmia Substrate during STAR
STAR’s critical requirements are developing a technology that can accurately identify the substrate and delineation the target, that is, anatomical localization and three-dimensional target reconstruction through imaging such as CT or MRI. Unlike tumor SBRT, which can identify and outline the target area only by imaging such as CT or MR, the arrhythmogenic target area depends on myocardial tissue’s electrical characteristics, so single imaging cannot fully identify the target substrate. The substrate of ventricular tachycardia is closely related to underlying heart disease. In ischemic cardiomyopathy, scar substrate is usually fused and limited to the corresponding distribution area of the diseased coronary artery. In non-ischemic cardiomyopathy, including non-ischemic dilated cardiomyopathy, myocarditis, and sarcoidosis, myocardial scars are usually less confluent with distributing throughout the mid myocardium or subepicardium [60,61]. Therefore, localization using non-invasive techniques can prove challenging. The origin of ventricular arrhythmias is usually associated with a myocardial scar or marginal areas identified as low voltage areas during intracardiac catheter mapping, and ECG shows fragmentation potential and late potential [4]. It was found that the late potential of endocardial catheter mapping of patients with coronary artery disease was up to 12% [62].
A conventional 12-lead body surface electrocardiogram can non-invasively diagnose and localize arrhythmias. Nevertheless, it can only measure several potentials from body surface point to obtain cardiac electrical signals, limiting specificity and sensitivity. Although the ECGI technique reported by Cuculich et al. [52], and Robinson et al. [48], can non-invasively map the ventricular tachycardia substrate, it is limited to recognizing epicardial depolarizing signals the ventricular tachycardia substrate originating from the endocardium or intraventricular wall may be ignored. Therefore, the substrate-based ablation method is not the best choice. At present, most of the patients receiving STAR had a history of catheter ablation with generating detailed epicardial or endocardial EAM data.
In May 2020, Brett et al. [63], established a workflow report on converting catheter-based electrophysiological mapping to DICOM. Brett et al. developed a unique MATLAB script to extract these data, converted to VTK format, used standard image processing software to visualize the heart structure, processed images through 3D Slicer open-source software package, and was compatible with the CARTO3 system.
Then, Hohmann et al. [64], proposed a novel high-precision target definition method. The multimodal integration of the electroanatomic map with the planning CT allows for highly accurate localization of previously identified electrophysiological features in CT space. Also, the software supports CARTO3, Ensite, and the RHYTMTAHDx heart mapping system. These imaging compatibilities further improve the Quality and reproducibility of image fusion and provide higher accuracy for STAR.
However, how to measure the ventricular tachycardia substrate non-invasively in patients who have not received catheter ablation before? It has been reported that ECVUETM [65], which integrates ECG imaging and anatomical imaging, can achieve high spatial mapping resolution. In this study, the diagnosis rate of 12-lead ECG intracardiac arrhythmias was only 76.2%, while the diagnosis rate of the ECVUETM system was as high as 95.2%. The sub- localized origin of ventricular arrhythmias in 12-lead ECG was even more inaccurate, with an accuracy of only 38.1%, while the accuracy of ECVUETM technology was 95.2%. This technique can locate the VT substrate more accurately, save operation time, and improve the curative effect and safety. However, this process requires simultaneous CT, which in turn increases the patient’s radiation exposure.
Selection of Dose in STAR
Unlike tumor SBRT, which adjusts single dose and radiation times according to tumor type, location, and surrounding risk organs, the vast majority of STAR choose only a single treatment dosing regimen with 25Gy in a fraction. Dose-finding studies for optimizing both safety and efficacy in STAR must be critical. In the first animal study, Sharma et al. [39], found that a single dose of at least 25Gy could create a lesion and alter electrophysiological properties of the tricuspid isthmus, atrioventricular node block, pulmonary vein-left atrial junction, and left atrial appendage with voltage decrease in the pig model. Subsequently, Maguire et al. [34], also confirmed that a single dose of 25-35Gy could induce transmural fibrosis and lead to electrical isolation six months after radiation in pulmonary veins of miniature pigs. Similarly, Blanck et al. [35], reported that transmural scar formation in porcine myocardial tissue could be induced six months after a single dose of 32.5Gy radiation. However, some studies have suggested that 40Gy is the lowest single prescription dose for electrophysiological effects such as atrioventricular block or pulmonary vein isolation [66]. Lehmann’s team [36] studied the responses of atrioventricular node, right superior pulmonary vein, left atrial junction, and left ventricular free wall to different doses of radiation in the pig model. Single-dose of 25Gy could induce slight fibrosis, whereas 40 and 55 Gy induced significant fibrosis, and there is no surrounding tissue damage during follow-up for six months. The single prescription dose is different in preclinical studies of different institutions, and the single-dose selection of SBRT is related to tissue sensitivity and target volume.
In clinical studies, Cuculich, Robinson et al. [48,50,52,55-57], reported that the single dose of 25Gy in target tissue had no obvious complications in the short term. The burden of ventricular tachycardia decreased significantly. However, compared to arteriovenous malformations, seizures, and other non-neoplastic diseases with a single dose lower than 20Gy, 25 Gy used to STAR is relatively high [27,28]. It is universally known that the radiation effect obeys the sigmoid dose-response after threshold dose activation in any tissue [67]. Therefore, there is a need to reduce the target dose to the minimal effective level capable of maintaining the efficacy of SBRT. Then, the exposure dose of surrounding normal tissues and risk organs will be reduced, which favors decreasing long-term complications. The ablation volume and prescribed dose are the main factors affecting unnecessary radiation, which need further exploration in preclinical and clinical studies. Most studies have reported the electrophysiological alterations of atrial tissue and atrioventricular node about radiation. However, the clinical studies related to the early electrophysiological changes of cardiomyocytes and long-term scar tissue progression after ventricular radiation are limited [Figure 4].
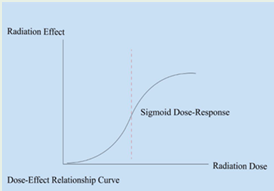
Figure 4: The curve between radiation dose and radiation effect.
Lesion pathophysiology after STAR
Because malignant tumor cells are rapidly proliferative, malignant tumors of SBRT can inhibit cell proliferation and induce apoptosis through direct or indirect DNA damage, interference with cell mitosis, and destruction of cell function. As terminally differentiated cells, cardiomyocytes are relatively resistant to the toxic side effect of radiation. Unlike catheter ablation that causes immediate coagulation necrosis and electrophysiological changes in an instant, SART induces a series of complex histological effects of acute and chronic cardiac cells, including microvascular endothelial injury, oxidative stress, inflammation, and fibrosis.
The mechanism of STAR injury in myocardial tissue is various, partly due to DNA double-strand break, which induces cardiomyocyte apoptosis. In contrast to cardiomyocytes, endothelial cells do proliferate and therefore are more sensitive. Radiation effects in the myocardium are mediated predominantly through microvascular endothelial insufficiency, chronic ischemia, fibrosis, and scar formation. The mechanism of injury for high doses of STAR is still less well known and debated. Some animal experiments showed that superoxide and peroxides in microvessels of rats increased significantly after radiation [68]. Another mechanism of human vascular inflammatory injury is via the activation of peroxide and nuclear factor-kappa B [69]. After SBRT of the mediastinal tumor, histology showed cardiomyocyte loss with eosinophil infiltration, vascular inflammation, ischemic necrosis [33]; TGF- β and IL-1 β stimulated fibroblast proliferation and collagen deposition induced by radiation, and finally achieved fibrosis [39].
In theory, the myocardial radiation effect mediated by microvascular endothelial system injury can not be observed until eight weeks after treatment. However, antiarrhythmic effects appeared in most patients within the first six weeks after STAR. Jumeau et al. [56], reported that when drug and catheter ablation were ineffective in treating VT, STAR could reduce VT burden in an emergency with a single dose of 25Gy. The episodes of VT conspicuously reduced within a few days. Also,in Cuculich and other series of studies [48,50,52], episodes of VT decreased significantly within the first month after STAR; the antiarrhythmic effect appeared to occur much earlier than the expected process of cardiomyocyte death and fibrotic replacement of high-dose radiation therapy, and the existing mechanism can not explain this early effect, which indicates that except for radiation-induced fibrosis, there are other unknown mechanisms. Histological findings after STAR showed edema and vacuolation of endothelial cells with mild fibrosis under the microscope in the treatment area. In addition, Lloyd et al. [53], observed that the intercalated disk or gap junction area of SBRT-treated regions was destroyed under electron microscope from cardiac transplant, which may explain the relatively acute treatment responses with a single high dose of 25Gy. Previous animal experiments found that STAR can change the gene expression pattern by alterations in connexin protein 43 expressions and distribution, enhancing electrical conductivity, reducing repolarization spatial dispersion, and can reduce the incidence of VA in the myocardial infarction rabbit model, which may help to explain the early effects after STAR [70]. However, the detailed pathological mechanism is not precise. Therefore, there is necessary to explore further the effects of high dose radiation on pathophysiology and molecular expression of ventricular tachycardia substrate. Further understanding of mechanisms of radiation on cardiac tissues will help improve STAR technology’s security and effectiveness [Figure 5].
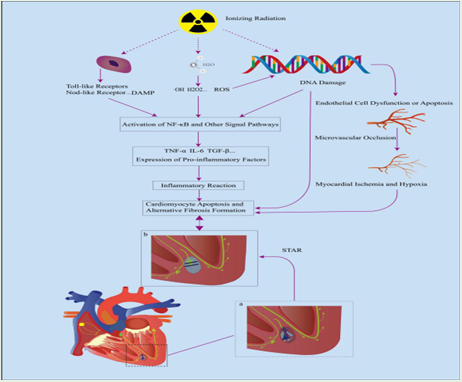
Figure 5: Biological effects of ionizing radiation on human myocardial tissue.green is the surrounding major organs at risk (including lungs, aorta, esophagus).
First of all, radiation may induce DNA double-strand breaks, production of reactive oxygen species, and release of the damage-associated molecular pattern (DAMP) in endothelial cells, jointly activate NF-κ B and other related signal pathways, promote the expression of pro- inflammatory factors such as TNF-α, IL-6, IL-8 and TGF-β in a time-and dose-dependent manner, aggravate the inflammatory response, and cause fibrotic transformation of viable myocardium in scar tissue. Secondly, ionizing radiation can directly destroy the DNA double- strand of cardiomyocytes, induce cardiomyocyte apoptosis and reduce the number of viable myocardium in the scar area. In addition, the proliferating endothelial cells are more sensitive to ionizing radiation, which can gradually cause endothelial cell dysfunction and microvascular occlusion, resulting in ischemia and hypoxia of cardiomyocytes in the scar area, and finally tend to apoptosis and fibrosis. In short, ionizing radiation can destroy the surviving cardiomyocytes in scar tissue, reduce abnormal electrical activity, interrupt the re- entrant circuit, and reduce the burden of arrhythmia [Figure 6].
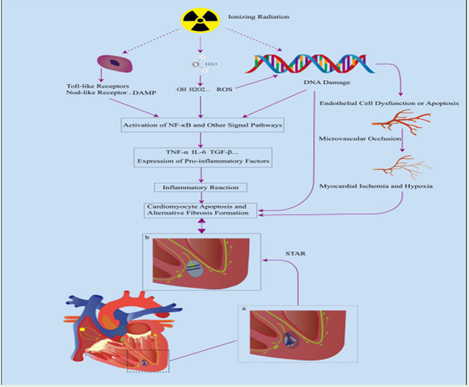
Figure 6: Effect of radiation on the gene expression pattern of myocardial fibers.
As terminally differentiated cells, cardiomyocytes have a specific resistance to ionizing radiation compared with vascular endothelial cells. However, radiation may induce changes in the gene expression pattern of cardiomyocytes by up-regulating the connexin 43, a low- resistance channel of gap junction in the intercalated disk structure between myocardial fibers, to improve the electrical conduction between viable myocardial fibers in scar tissue and reduce the heterogeneity of spatial repolarization and bring down the susceptibility to ventricular arrhythmias.
PERSPECTIVES
In theory, STAR can ablate the substrate in any part of the heart, which has the advantages of being short time and relatively non-invasive. Nevertheless, STAR has been mainly used in patients with refractory ventricular tachycardia who have failed traditional catheter ablation or have contraindications. Most of them have a relatively short expected survival time. Overall, small samples of prospective or retrospective clinical studies have been reported to show that patients are safe and effective during short-term follow-up; however, previous SBRT studies of mediastinal tumors have found that the onset of radiation- related cardiotoxicity is significantly later than that of most clinical studies. Therefore, within the scope of ethics, it is necessary to include a broader and larger group of patients to conduct a large cohort, multicenter prospective study, long term follow-up after the operation, and improve the data evaluation of long-term safety and efficacy.
STAR has a bright future, but there are differences among different research institutions in substrate location, target delineation or radiation times, and single-dose selection. There is no clear expert consensus or unified guidelines. Therefore, further clinical exploration is needed in the future, such as optimizing imaging, developing dedicated STAR delivery technology, creating new treatment flow, improving accurate target delivery, and minimizing the risk of surrounding tissues and organs. In addition, close communication and cooperation between radiotherapy departments, oncology radiology departments, and cardiac electrophysiologists are essential. Whether this technique can become a first-line treatment of cardiac arrhythmia still needs to be verified by the long-term safety and effectiveness of more clinical data of patients. At present, clinical studies tend to explore the mechanism of delayed effects of STAR, but there are few reports on the evolution of early biological effects of myocardial tissue. In addition to further obtaining long-term clinical data, it is necessary to study the potential antiarrhythmic mechanism of STAR. STAR is widely used in arrhythmias. It also explores the treatment of other cardiac diseases, such as hypertrophic obstructive cardiomyopathy and hypertensive plexus radiofrequency ablation.
How to Cite
References
URL: https://pubmed.ncbi.nlm.nih.gov/28625728/
URL: https://pubmed.ncbi.nlm.nih.gov/28457244/
URL: https://pubmed.ncbi.nlm.nih.gov/30995375/
URL: https://pubmed.ncbi.nlm.nih.gov/19573735/
URL: https://pubmed.ncbi.nlm.nih.gov/19348944/
URL: https://pubmed.ncbi.nlm.nih.gov/31075787/
URL: https://pubmed.ncbi.nlm.nih.gov/29173411/
URL: https://pubmed.ncbi.nlm.nih.gov/31444267/
URL: https://pubmed.ncbi.nlm.nih.gov/31631881/
URL: https://pubmed.ncbi.nlm.nih.gov/24345399/
URL: https://pubmed.ncbi.nlm.nih.gov/26320108/
URL: https://pubmed.ncbi.nlm.nih.gov/11827924/
URL: https://pubmed.ncbi.nlm.nih.gov/18768944/
URL: https://pubmed.ncbi.nlm.nih.gov/18768943/
URL: https://pubmed.ncbi.nlm.nih.gov/27149033/
URL: https://pubmed.ncbi.nlm.nih.gov/27733494/
URL: https://pubmed.ncbi.nlm.nih.gov/28167089/
URL: https://pubmed.ncbi.nlm.nih.gov/28506916/
URL: https://pubmed.ncbi.nlm.nih.gov/23414740/
URL: https://pubmed.ncbi.nlm.nih.gov/21540439/
URL: https://pubmed.ncbi.nlm.nih.gov/21540439/
URL: https://pubmed.ncbi.nlm.nih.gov/19660291/
URL: https://pubmed.ncbi.nlm.nih.gov/21699857/
URL: https://pubmed.ncbi.nlm.nih.gov/7946448/
URL: https://pubmed.ncbi.nlm.nih.gov/27932046/
URL: https://pubmed.ncbi.nlm.nih.gov/20589114/
URL: https://pubmed.ncbi.nlm.nih.gov/25414830/
URL: https://pubmed.ncbi.nlm.nih.gov/21121803/
URL: https://pubmed.ncbi.nlm.nih.gov/28367392/
URL: https://pubmed.ncbi.nlm.nih.gov/28367392/
URL: https://pubmed.ncbi.nlm.nih.gov/22340985/
URL: https://pubmed.ncbi.nlm.nih.gov/3384719/
URL: https://pubmed.ncbi.nlm.nih.gov/20156591/
URL: https://www.cureus.com/articles/34-cardiac-radiosurgery-cyberheart-for-treatment-of-arrhythmia-physiologic-and-histopathologic-correlation-in-the-porcine-model#!/
URL: https://pubmed.ncbi.nlm.nih.gov/24751407/
URL: https://pubmed.ncbi.nlm.nih.gov/28408649/
URL: https://pubmed.ncbi.nlm.nih.gov/17341728/
URL: https://pubmed.ncbi.nlm.nih.gov/16360786/
URL: https://pubmed.ncbi.nlm.nih.gov/12408314/
URL: https://pubmed.ncbi.nlm.nih.gov/8760008/
URL: https://pubmed.ncbi.nlm.nih.gov/23484825/
URL: https://pubmed.ncbi.nlm.nih.gov/8411552/
URL: https://pubmed.ncbi.nlm.nih.gov/27919338/
URL: https://pubmed.ncbi.nlm.nih.gov/30592114/
URL: https://pubmed.ncbi.nlm.nih.gov/26487757/
URL: https://pubmed.ncbi.nlm.nih.gov/8120544/
URL: https://pubmed.ncbi.nlm.nih.gov/28721895/
URL: https://pubmed.ncbi.nlm.nih.gov/30586734/
URL: https://pubmed.ncbi.nlm.nih.gov/30586734/
URL: https://pubmed.ncbi.nlm.nih.gov/31121018/
URL: https://www.cureus.com/articles/2533-cardiac-radiosurgery-for-malignant-ventricular-tachycardia#!/
URL: https://pubmed.ncbi.nlm.nih.gov/31585181/
URL: https://pubmed.ncbi.nlm.nih.gov/31585181/
URL: https://pubmed.ncbi.nlm.nih.gov/32151737/
URL: https://pubmed.ncbi.nlm.nih.gov/32803639/
URL: https://pubmed.ncbi.nlm.nih.gov/29753550/
URL: https://pubmed.ncbi.nlm.nih.gov/32657082/
URL: https://pubmed.ncbi.nlm.nih.gov/27660737/
URL: https://pubmed.ncbi.nlm.nih.gov/32071622/
URL: https://pubmed.ncbi.nlm.nih.gov/28258845/
URL: https://pubmed.ncbi.nlm.nih.gov/27392945/
URL: https://pubmed.ncbi.nlm.nih.gov/3948367/
URL: https://pubmed.ncbi.nlm.nih.gov/32416269/
URL: https://pubmed.ncbi.nlm.nih.gov/32648343/
URL: https://pubmed.ncbi.nlm.nih.gov/25349226/
URL: https://pubmed.ncbi.nlm.nih.gov/25736725/
URL: https://pubmed.ncbi.nlm.nih.gov/25113761/
URL: https://pubmed.ncbi.nlm.nih.gov/16322529/
URL: https://pubmed.ncbi.nlm.nih.gov/20298931/
URL: https://pubmed.ncbi.nlm.nih.gov/17054928/