Abstract
Advances in primary cardiovascular prevention depend upon enhanced risk stratification. Gated coronary artery calcium CT scoring independently stratifies the risk for major acute cardiac events including sudden death. Low-dose aspirin use guided by such scoring has been recommended to reduce the transiently increased marathon-related risk for cardiac arrest in middle-aged men due mainly to atherosclerotic coronary artery disease. This measure is supported by a 44% reduction in first heart attacks in same-aged men in the final report on aspirin in the Physicians’ Health Study, a randomized controlled primary prevention trial. This strategy may also attenuate the age-dependent increased risk for sudden cardiac death during recreational sports activity in older persons. This same approach may furthermore mitigate the excess cardiovascular risk in conditions in which inflammation promotes progressive coronary atherosclerosis. Human immunodeficiency virus infection, myalgic encephalomyelitis/chronic fatigue syndrome and long Covid exemplify such diagnoses. Such use is supported by a 31% decrease in major acute cardiac events in persons at moderate risk with the addition of aspirin to the polypill in TIPS-3, a randomized controlled primary prevention trial. Inexpensive and readily available worldwide, guided low-dose aspirin use for enhanced primary cardiovascular prevention in clinical practice may ameliorate the risk of sudden cardiac deaths in persons with subclinical atherosclerotic coronary artery disease, which is the presenting symptom in up to 40% of cases.
Keywords
INTRODUCTION
The rationale for aspirin use guided by coronary artery calcium scoring was initiated for reducing the transiently elevated risk for cardiac arrest and sudden death during marathons mainly in middle-aged men with subclinical atherosclerotic coronary artery disease [1-4]. Such aspirin use is supported by a 44% reduction in first heart attacks in middle-aged men in the final report on aspirin in the Physicians’ Health Study, a randomized controlled primary prevention trial [5]. This intervention is furthermore consistent with the current guidelines of the American Heart Association and the American College of Physicians for primary prevention in persons identified at high risk [6].
An incidence of such events remained the same from 2010-2023 compared to 2000–2009, although fatalities decreased due to incorporating proficient cardiopulmonary resuscitation services with automated external defibrillators along race courses [7,8]. Beyond reducing the risk for cardiac arrest in marathon runners with a subclinical atherosclerotic coronary heart disease, this same strategy may also mitigate the increasing age-dependent risk for exertional sudden cardiac death during recreational sports activity in older persons [9,10].
Beyond reducing risk for exertional cardiac arrest during sports activity, this approach may additionally be appropriate for patients with illnesses in which inflammation promotes progressive coronary atherosclerosis. Autoimmune disorders Including rheumatoid arthritis, human immunodeficiency virus infection, myalgic encephalomyelitis/chronic fatigue syndrome and possibly long Covid exemplify diagnoses in which cardiovascular risk is heightened by this mechanism. Such usage is supported by a 31% decrease in major acute cardiac events in individuals at moderate risk with the addition of aspirin to the polypill in TIPS-3, a randomized controlled primary prevention trial [10].
Aspirin–use as guided by coronary artery calcium scoring for primary cardiovascular prevention may additionally be relevant for patients with serious psychiatric illness such as schizophrenia, which confers a several-fold increased risk for sudden cardiac death and reduces like expectancy by more than 10 year [11,12]. Inexpensive and readily available worldwide, such aspirin use may serve to reduce the disparities in access to preventive cardiovascular services due to stigma in such patients. Sequential monitoring with carotid ultrasonography may reliably identify patients at progressively increasing risk [13,14], who might benefit the most from this intervention in the absence of contraindications.
Table 1: Coronary Artery calcium scores and the anticipated benefit of enhanced primary prevention with low dose pre-race aspirin for reducing the risk of marathon-related cardiac arrest
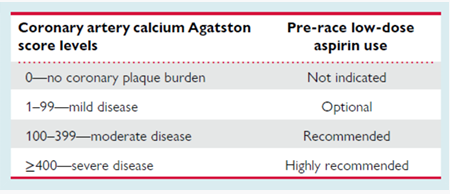
Reproduced from: Siegel A. Pre-race aspirin to attenuate the risk for marathon-related cardiac arrest: deconstructing the legacy of Pheidippides. Eur Heart J. 2023, ehad641. (Ref 2)
Beyond using this intervention for patients with enhanced cardiovascular risk due to specific diagnoses, aspirin use guided by coronary artery calcium scoring might be readily incorporated into clinical practice, providing actionable information on a client’s proximate cardiovascular risk beyond that based on conventional risk calculators [15]. Frontline clinicians may thereby participate in mitigating unexpected cardiac arrests, which are the presenting symptom of this disease in up to 40% of fatalities [16]. Primary care providers in the trenches may contribute to reducing the daunting burden of atherosclerosis, which is projected by the American Heart Association to increase to 2050 [17].
CONCLUSION
Risk-based decision making is foundational to the prevention of atherosclerotic cardiovascular disease. Aspirin use guided by coronary artery calcium scoring is evidencebased for primary prevention of major acute cardiac events including sudden death in persons with subclinical atherosclerotic coronary artery disease. This approach is supported by current guidelines of the American Heart Association and the American College of cardiology, which recommend aspirin for persons at high risk.
TAKE-AWAY POINTS
1. Coronary artery calcium scoring independently stratifies the risk for major acute cardiovascular events including sudden cardiac death
2. Low-dose aspirin has been demonstrated to be significantly cardioprotective in two randomized controlled primary prevention trials
3. Low-dose aspirin use is approved for primary cardiovascular prevention in current guidelines of the American Heart Association and the American College of Cardiology
How to Cite
References
URL: https://pubmed.ncbi.nlm.nih.gov/36871752/
URL: https://pubmed.ncbi.nlm.nih.gov/37847804/
URL: https://pubmed.ncbi.nlm.nih.gov/30296406/
URL: https://esmed.org/MRA/mra/article/view/3741
URL: https://www.nejm.org/doi/full/10.1056/NEJM198907203210301
URL: https://pubmed.ncbi.nlm.nih.gov/30894318/
URL: https://jamanetwork.com/journals/jama/fullarticle/2832121
URL: https://www.nejm.org/doi/full/10.1056/NEJMoa1106468
URL: https://pubmed.ncbi.nlm.nih.gov/19318955/
URL: https://europepmc.org/article/PMC/PMC8756014
URL: https://pubmed.ncbi.nlm.nih.gov/39832344/
URL: https://pubmed.ncbi.nlm.nih.gov/39438152/
URL: https://pubmed.ncbi.nlm.nih.gov/39357937/
URL: https://pubmed.ncbi.nlm.nih.gov/39674300/
URL: https://www.jacc.org/doi/10.1016/j.jacep.2024.12.012
URL: https://www.ahajournals.org/doi/10.1161/CIR.0000000000001256