Abstract
Objective: The purpose of our study is to describe a new imaging finding observed on CT Angiography (CTA), namely the thicker-wall sign of Acute Aortic Dissection (AAD), which makes it easier to locate the true lumen of AAD.
Conclusion: The thicker-wall sign of the true lumen of AAD could be directly displayed on CTA. The identification of this sign can reliably differentiate the true lumens from AAD, which is beneficial for timely and accurately assessing the impact of the aortic dissection on the various branch arteries.
ANATOMY OF AORTA
The aorta wall comprises three layers: the intima, media, and adventitia. The intima is the innermost layer, composed of a single layer of endothelial cells on a basement membrane that provides a smooth surface for blood flow and is separated from the media by the internal elastic lamina.The elastin-rich and smooth muscle-rich media is the thickest layer, enabling the aorta to expand and contract. The adventitia is the outermost layer and contains an external elastic membrane, connective tissue, and perivascular nerves that provide additional support and structure to the aorta [1]. The vasa vasorum are small vessels composed of endothelial and smooth muscle cells, distributed in the outer 1/3 layer of the aortic wall, penetrating the aortic wall from the outer adventitia to perfuse the outer aortic wall and a substantial portion of the media [2] (Figure 1).
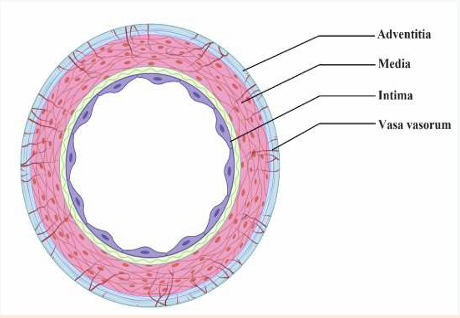
Figure 1: Schematic of normal aortic wall. The layers of the normal aortic wall consist of the intima, the media, and the adventitia
MECHANISM OF AORTIC DISSECTION
Acute Aortic Dissection (AAD) is a highly fatal cardiovascular emergency and has an estimated incidence of between 4.5 and 7 per 100,000 [3]. The main cause of AAD is a tear in the degeneration of the aortic media, which results in a blood column entering the medial layer of the aorta causing a ‘hydraulic endarterectomy’, creating an intimomedial dissection flap of medial and intimal aortic tissue that separates the aorta’s true and false lumens [4,5]. The structural weakness of the aortic wall and increased wall tension on the aortic wall, combined with elevated blood pressure, are the main causes of aortic dissection [6]. The tear usually dissects the media in two parts, forming a new false lumen between the intima-media and media-adventitia (Figure 2). The intimomedial flap consists of the aortic intima and the inner 2/3 of the media. The true lumen is lined by the intima, while the false lumen is located within the media.
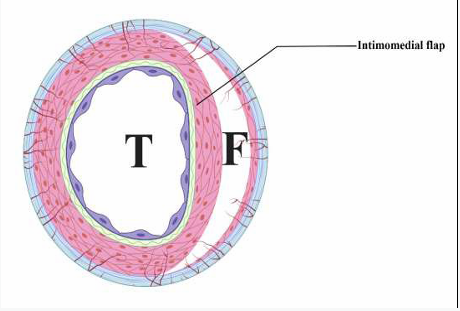
Figure 2: Schematic of AAD. AAD is defined as the separation of the medial lamellar units, a tear in the intima layer results in blood entry to the media layer, developing in an intimomedial flap and dividing the original vessel into true lumen (T) and false lumen (F).
This separate false lumen for blood flow is externally bound only by the outer 1/3 of the media and the adventitia [7-9].
IMAGING BASIS OF THE THICKER-WALL SIGN
It is based on this anatomical foundation that we propose a sign for distinguishing true and false lumen - the thicker-wall sign. The intimomedial flap is composed of the aortic intima and the inner 2/3 of the media, and its thickness is closer to 3/4 of the initial aortic wall thickness. This means that the true lumen has a relatively complete and thicker-wall. The distance between calcified spots on the mural flap was shortened within AAD, confirming that the mural flap had contracted post-dissection, further supporting the theory of thicker-wall of the true lumen [10]. The thinner outer wall of the false lumen contains approximately one-third of the elastin it contained at baseline. The outer diameter of the aorta will expand due to the expansion and extension of the false lumen, further promoting the stretching and thinning of the false lumen wall within AAD. This means that the false lumen has a thinner wall. In addition, due to the formation of atherosclerotic plaque and calcified plaque on the intima, the true lumen side of the intimal valve is often rougher, while the false lumen side is relatively smoother, which is also helpful for the discovery of the thicker-wall sign (Figure 3A, 3B).
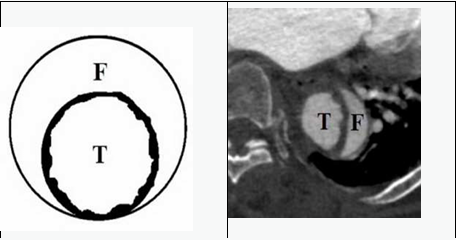
Figure 3: (A) Schematic display of the thicker-wall sign of AAD. (B) CTA in the axial plane shows the thicker-wall sign of AAD, which is the thicker-wall surrounding the true lumen and the true lumen side of the intimal valve is not smooth, while the wall of false lumen is thin ner and relatively smooth. T, true lumen; F, false lumen.
Clinical Practice of the Thicker-Wall Sign
As the false lumen gradually expands, the true lumen is gradually compressed, producing different shapes, and even collapsing or intima-intussusception may occur (Figure 4).
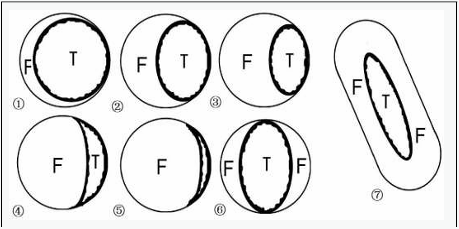
Figure 4: Schematic diagram of aortic dissection with different manifestations of true and false lumens. As the false lumen gradually expands, the true lumen compresses ( ① - ④ ), and even collapses ( ⑤ ). Complex Aortic dissection, the intima-intussusception AD can occasionally be found (⑥, ⑦). F=false lumen, T=true lumen.
The most reliable imaging stan dard is to identify the continuity between the true lumen of AAD and the unaffected lumen of the proximal or distal aortic portion of the dissection [11]. We found that the thicker-wall sign is applicable to the manifestations of these types of true lumen, and it is almost possible to completely distinguish true lumen using this sign only within the axial imagines (Figure 5).This sign can be quickly mastered and easily applied, and is not only applicable to most levels of the aorta, including the aortic arch level, but also to the level of branch issuance (Figure 5C). The study was approved by the medical ethics committees of the Third Affiliated Hospital of Xinxiang Medical University and adhered to the principles of the Declaration of Helsinki (Ethical Review No.: 2023-030-01).
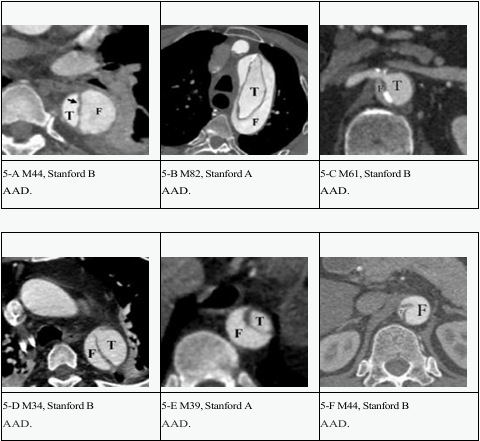
Figure 5: (A-F). Spectrum of the thick wall sign of the true lumen in different forms of different patients with AAD on CTA. F=false lumen, T=true lumen.
LIMITATIONS
However, the application of this sign has certainlimitations. For instance, the false lumen wall may be poorly visualized in cases of intraluminal thrombosis or insufficient contrast agent filling in the false lumen. It should be emphasized that delayed phase scanning plays an important role in the diagnosis of aortic dissection. Thrombosis in the false lumen may be overestimated when only arterial imaging is relied on. At the same time, delayed phase imaging is also helpful to identify thickened wall signs (Figures 6-A and 6-B).
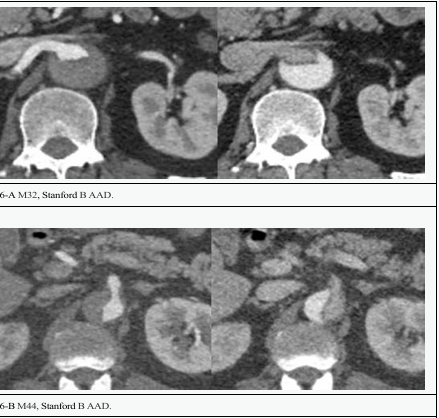
Figure 6: Delayed phase imaging of the thickened wall signs.
Moreover, in younger AAD patients without significant atherosclerosis, the detectability of the sign may be reduced. In this situation, we can also identify the false lumen through supplementary signs such as smoother intimomedial flap on one side, intraluminal thrombus, cobweb sign, outer wall calcification, eccentric flap calcification and contrast agent opacity with the false lumen, in order to identify the true lumens more quickly and accurately, and to judge the relationship between branches and the true and false lumens [11,12].
In short, we suggest that the thicker-wall sign displayed on CTA is an imaging finding that is consistent with true lumen recognition and can be used for imaging diagnosis of AAD.
AUTHOR CONTRIBUTIONS
Wenhua Guan conceived the idea and with Jinping Li, wrote the first draft of the manuscript. All authors have read and approved the final version of this manuscript and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All persons designated as authors qualify for authorship, and all those who qualify for authorship are listed.
DECLARATIONS
Funding Information
Henan Provincial Medical Science and Technology Research Plan, Henan Provincial
Health and Family Planning Commission (2018020378).
Henan Provincial Medical Science and Technology Research Plan, Henan Provincial Health Commission (LHGJ20230544).
Key Laboratory of Imaging Diagnosis of Aortic Diseases in Xinxiang City.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available due to patients’ privacy but are available from the corresponding author on reasonable request.
Informed Consent Statement
Additional informed consent was obtained from all individual participants for whom identifying information is included in this article.