Abstract
Aortic stenosis (AS) is a high-afterload state, often leading to compensatory left ventricular (LV) hypertrophy and diastolic dysfunction due to long term microscopic and macroscopic adaptive changes. The impact of surgical aortic valve replacement (SAVR) has traditionally been well studied in this patient population, with reports showing improved hemodynamics, diastology and LV regression post surgical correction. The
corresponding effects have not been adequately mapped amongsimilar patients undergoing transcatheter aortic valve replacement (TAVR). Herein, we report a case that traces the paradoxical changes that occur in both diastolic function and LV regression in a patient after TAVR. Thereafter, we correlate the physiologic findings with the oft understudied microscopic and reverse adaptive changes post valve replacement.
Keywords
Introduction
Aortic stenosis (AS) is a high-after load state, often leading to compensatory left ventricular (LV) hypertrophy and diastolic dysfunction [1]. Studies in patients with severe AS have demonstrated adaptive microscopic changes, with progressive cardiomyocyte hypertrophy, extracellular matrix (ECM) expansion and interstitial fibrosis caused by collagen deposition [2,3]. The impact of surgical aortic valve replacement (SAVR) on these microscopic as well as macroscopic changes has been well reported. While normalization of LV hypertrophy is not seen among these patients, they typically undergo considerable LV regression with concordant improvement in diastolic function post procedure [4-6]. The extent and sustainability of these changes is largely unknown in patients with pure AS undergoing transcatheter aortic valve replacement (TAVR). Given the increased utilization of TAVR in the management of patients with severe AS and improved survival, there is emerging interest if similar effects on diastolic function are seen among these patients. Herein, we review a patient with severe AS who underwent TAVR and correlate the effects of TAVR on LV remodeling and diastolic function overtime, compared to the changes expected in patients undergoing SAVR.
Case Presentation
An 81 year-old female patient with severe symptomatic aortic stenosis presented for TAVR evaluation to our institution, due to an elevated surgical risk. Pre-operative transthoracic echocardiogram (TTE) confirmed the severity of AS and impaired diastolic function (Table 1). She underwent transfemoral TAVR with a 23 mm Edwards Sapien 3 valve. She was discharged on post-operative day 2 with no complications. There was significant improvement in the diastology parameters at one month post-TAVR, along with improvement in LVH as seen by decrease in LV mass index, interventricular septum and posterior wall thickness (Table 1). However, comparative TTE at one year revealed lack of sustenance of these changes with reversal of the initially favorable findings (Figure 1).
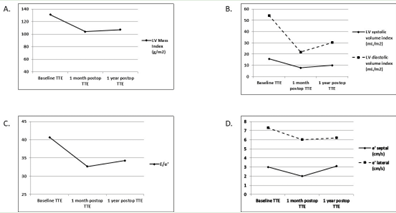
Figure 1: Left ventricular reverse remodeling overtime post-TAVR. Note: A) Indexed LV mass; B) Indexed LV diastolic (dashed line) and systolic (solid line) volume; C) E/e’ ratio; D) Lateral (dashed line) and septal (solid line) e’.
Table 1: Changes overtime after TAVR by transthoracic echocardiography.
|
TTE parameters |
Baseline TTE |
1 month post-operative TTE |
1 year post-operative TTE |
|
Aortic valve |
|||
|
Valve area (cm2) |
0.84 |
1.6 |
1 |
|
Mean gradient (mmHg) |
51 |
17 |
10.5 |
|
Peak AV velocity (cm/s) |
465 |
240.5 |
214 |
|
Dimensionless index |
0.25 |
0.71 |
0.55 |
|
LV ejection fraction (%) |
70-74 |
>75 |
>75 |
|
LV diastolic function |
|||
|
Grade of diastolic dysfunction |
2 |
Indeterminate |
2 |
|
MV E/A |
0.9 |
0.4 |
0.8 |
|
MV E velocity (cm/s) |
122 |
65.3 |
106.3 |
|
MV E/e’ |
40.67 |
32.65 |
34.29 |
|
MV septal e’ (cm/s) |
3 |
2 |
3.1 |
|
MV lateral e’ (cm/s) |
7.3 |
6 |
6.2 |
|
LAVI (mL/m2) |
59.3 |
22.3 |
29 |
|
TR velocity (cm/s) |
323.3 |
246.6 |
287 |
|
Aortic regurgitation |
None |
None |
Trace |
|
Mitral regurgitation |
Mild |
Trace |
None |
|
LV Volumetrics |
|||
|
LV systolic volume index (mL/m2) |
15.7 |
7.7 |
10 |
|
LV diastolic volume index (mL/m2) |
54.3 |
21.8 |
30.2 |
|
LV end-diastolic diameter (cm) |
3.8 |
4.1 |
4.4 |
|
LV end-systolic diameter (cm) |
2.1 |
2.5 |
3 |
|
Interventricular septum (cm) |
1.6 |
1.4 |
1.2 |
|
Posterior wall (cm) |
1.1 |
1.4 |
1.4 |
|
LV mass index (g/m2) |
131 |
104 |
107 |
|
Pulmonary artery systolic pressure (mm Hg) |
54 |
27 |
36 |
Note: AV, aortic valve; LAVI, left atrial volume index; LV, left ventricle; MV, mitral valve; TR, tricuspid regurgitation; TTE, transthoracic echocardiogram.
Discussion
Patients with AS have a fixed, high-afterload state with resultant LV remodeling due to myocardial hypertrophy, ECM expansion and interstitial fibrosis [2,3]. These structural changes consequentially cause hemodynamic derangement and diastolic function impairment [4,7]. Studies in patients with severe AS undergoing SAVR have demonstrated a favorable improvement in LV volumetrics with sequential histologic and imaging analyses showing LV regression within 6 months post procedure [5,6,8-11]. It is unknown if similar effects are seen in TAVR patients given the smaller valve sizes and higher mean gradients post-operatively.
In our case, despite several parameters of diastolic function demonstrating improvement in the immediate post-TAVR period, this improvement was not sustained at one year, revealing a lack of durability of the LV remodeling and diastology changes seen post-TAVR. There are multiple proposed mechanisms to explain these findings. One potential mechanism is nullification of the relief in valvular afterload by post procedural increase in supra valvular afterload in the form of arterial hypertension [12]. Another mechanism explaining the return of diastolic dysfunction at one year is the temporally disproportionate microscopic adaptive changes post procedure. Classically, the LV hypertrophic process is thought to be composed chiefly of sarcomeres laid down in parallel resulting in concentric hypertrophy. The hypertrophy is governed by sarcomere upregulation by increased mRNA activity as well as by collagen deposition and perimysial fiber increase by metal metalloproteinase (MMP’s) and tissue inhibitors of MMP’s (TIMP’s) activity. These signaling pathways presiding over myocytes and ECM are distinct and expressed at dissimilar rates resulting in asymmetrical LVH regression post-AVR. mRNA signaling following abrupt relief of afterload is halted immediately post procedure, in stark contrast to MMP activity which, inhibited by TIMP’s, is activated late and then incompletely [13,14]. The resultant effect is “accelerated” myocyte atrophy but with a more preserved interstitial composition that serves to hamper the expected regression of LVH [9]. Similar findings have been demonstrated in severe AS patients undergoing SAVR with serial cardiac MRI studies, where significant benefits in LV structure and function are noted up to 4 years post-SAVR, however still do not result in complete resolution of LVH and fibrosis, even in non hypertensive patients [6,9].
In summary, patients with severe AS undergoing SAVR experience a rapid, temporally relatable regression of LVH post surgery, with adjunct improvement in LV volumetrics and diastology. While the regression and hemodynamic correction is expected post TAVR as well, there is lack of durability of these changes. The case described above illustrates the paradoxical decline in LV diastolic function after an initial improvement post-TAVR due to inability of the microscopic adaptive changes to sustain themselves. More studies are needed on the long term trajectory of LV remodeling and diastology post TAVR along with clinical correlation of the same. This case is illustrative of the paradoxical temporal diastolic response post TAVR and should serve to remind the growing TAVR teams of this phenomenon.
How to Cite
References
URL: https://www.ncbi.nlm.nih.gov/pubmed/10908222
URL: https://www.ncbi.nlm.nih.gov/pubmed/20633819
URL: https://www.ncbi.nlm.nih.gov/pubmed/8028011
URL: https://www.ncbi.nlm.nih.gov/pubmed/21272899
URL: https://www.ncbi.nlm.nih.gov/pubmed/29471937
URL: https://www.ncbi.nlm.nih.gov/pubmed/16103240
URL: https://www.ncbi.nlm.nih.gov/pubmed/21865229
URL: https://www.ncbi.nlm.nih.gov/pubmed/21492429
URL: https://jcmr-online.biomedcentral.com/articles/10.1186/1532-429X-15-39
URL: https://www.ncbi.nlm.nih.gov/pubmed/15896607
URL: https://www.ncbi.nlm.nih.gov/pubmed/15558223
URL: https://www.ncbi.nlm.nih.gov/pubmed/15489093